
Ear injuries are the leading cause of morbidity among scuba divers. The most common injury is middle-ear barotrauma (MEBT). Most cases of MEBT are mild, heal spontaneously and are never reported. In more serious cases, divers seek medical attention, and some call DAN. Various surveys indicate that more than 50 percent of all divers experience MEBT at least once. In contrast, only 4.4 percent of divers experience DCS in their lifetime.
Divers are affected by various other ear injuries, many of which are preventable, detailed in the chapter that follows.
In this chapter, you’ll learn about:
- Middle-Ear Barotrauma
- Perforated Eardrum
- Inner-Ear Barotrauma
- Perilymph Fistula
- Alternobaric Vertigo
- Reverse Squeeze
- Facial Baroparesis
- TMJ
- Surfer’s Ear
- Swimmer’s Ear
Middle-Ear Barotrauma (MEBT)
Middle-ear barotrauma is the accumulation of fluid and blood in the middle ear or rupture of the eardrum as a consequence of failed equalization of pressure in the air space of the middle ear during diving or flying.
Mechanisms
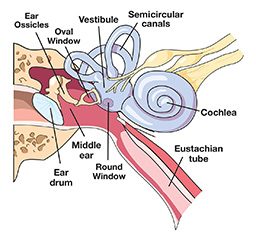
The air pressure in the tympanic cavity — air-filled space in the middle ear — must be equalized with the pressure of the surrounding environment. The Eustachian tube connects the throat with the tympanic cavity and provides passage for gas when pressure equalization is needed. This equalization normally occurs with little or no effort. Various maneuvers, such as swallowing or yawning, can facilitate the process.
An obstruction in the Eustachian tube can lead to an inability to achieve equalization particularly during a descent when the pressure changes fast. If the pressure in the tympanic cavity is lower than the pressure of the surrounding tissue, this imbalance results in a relative vacuum in the middle ear space. It causes tissue to swell, the eardrum to bulge inward, leakage of fluid and bleeding of ruptured vessels. At a certain point an active attempt to equalize will be futile, and a forceful Valsalva maneuver may actually injure the inner ear. Eventually, the eardrum may rupture; this is likely to bring relief from the pain associated with MEBT, but it is an outcome to be avoided if possible.
Factors that can contribute to the development of MEBT include the common cold, allergies or inflammation — conditions that can cause swelling and may block the Eustachian tubes. Poor equalization techniques or too rapid descent may also contribute to development of MEBT.
Manifestations
Divers who cannot equalize middle-ear pressure during descent will first feel discomfort in their ears (clogged ears, stuffed ears) that may progress to severe pain. Further descent only intensifies the ear pain, which is soon followed by serous fluid buildup and bleeding in the middle ear. With further descent, the eardrum may rupture, providing pain relief; this rupture may cause vertigo, hearing loss and exposure to infection.
Management
While diving: When feeling ear discomfort during descent, you should stop descending and attempt equalization. If needed, ascend a few feet to enable equalization. If equalization cannot be achieved, you should safely end the dive.
First aid: When feeling fullness in one’s ears after diving, abstain from further diving. Use a nasal decongestant spray or drops. This will reduce the swelling of nasal mucosa and Eustachian tube mucosa, which may help to open the Eustachian tube and drain the fluid from the middle ear. Do not put any drops in your ear.
Treatment: Seek a physician evaluation if fluid or blood discharge from the ear canal is present or if ear pain and fullness lasts more than a few hours. If vertigo and dizziness are present, which may be a symptom of inner-ear barotrauma, you should seek an urgent evaluation. Severe vertigo and nausea after diving require emergency medical care.
Fitness to Dive
Return to diving may be considered if a physician determines that the injury is healed and the Eustachian tube is functional.
Prevention
- Do not dive with congestion or cold.
- Descend slowly. If unable to equalize after a few attempts, safely end the dive to avoid significant injury that may prevent you from diving the rest of the week.
Tympanic Membrane Rupture (Perforated Eardrum)
Tympanic membrane perforation is a tear of the eardrum, which can occur while scuba diving due to failed middle-ear pressure equalization.
Mechanism
The tympanic membrane (TM) is a tissue separating the external ear from the middle-ear space. It is attached to a chain of small bones (auditory ossicles) located in the middle ear. The TM also serves as a barrier between the sterile middle-ear space and the ambient environment.
Eardrum rupture may be caused by descending without equalizing the pressure in the middle ear, by a forceful Valsalva maneuver, explosion, a blow to the ear/head, or acoustic trauma. It is usually accompanied with pain; rupture relieves the pressure (and pain) in the middle ear and may be followed by vertigo. There may be some bleeding in the ear canal.
Contributing factors include congestion, inadequate training and excessive descent rates.
Manifestations
- Ear pain during descent that stops suddenly
- Clear or bloody drainage from ear
- Hearing loss
- Ringing in the ear (tinnitus)
- Spinning sensation (vertigo)
- Nausea or vomiting that can result from vertigo
Management
Most perforated eardrums will heal spontaneously within a few weeks. It may be necessary to treat nasal and sinus congestion. If the tear or hole in your eardrum does not heal by itself, treatment will involve procedures to close the perforation. These may include:
- Eardrum patch: An ENT specialist may seal the tear or hole with a paper patch. This is an office procedure in which an ENT applies a chemical to the edges of the tear to stimulate growth and then applies a paper patch over the hole to provide a support structure for the growth of eardrum tissue.
- Surgery: Large eardrum defects may be fixed by surgery (tympanoplasty). An ENT surgeon takes a tiny patch of your own tissue and plants it over the hole in the eardrum. This procedure is done on an outpatient basis, meaning you can usually go home the same day unless medical conditions require a longer hospital stay.
For an ENT referral in your area, email or call the DAN Medical Information Line at +1 (919) 684-2948.
Fitness to Dive
If your physician feels the healing is solid and there is no evidence of Eustachian tube problems, you can return to diving within several months. Chronic perforations that do not heal are a contraindication to diving.
Prevention
Do not dive with congestion. Maintain a comfortable rate of descent, and equalize as needed.
O’Neill Grading System
The O’Neill grading system is a new way to grade the severity of middle-ear barotrauma. It is simplified and is expected to provide more consistent diagnosis with sufficient details to direct the treatment.
Grade 0
Eustachian Tube Dysfunction
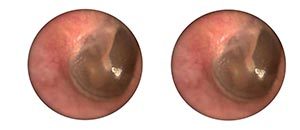
- Baseline photo depicting anatomical appearance of the TM before exposure to pressure
- Symptoms with no anatomical change (no trauma) from baseline
Grade 1
Barotrauma
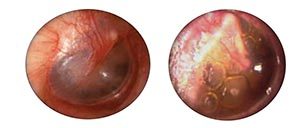
- Erythema increased from baseline
- Fluid or air trapping (visible bubble) in the middle-ear space
Grade 2
Barotrauma
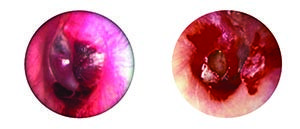
- Any bleeding noted within the tympanic membrane or middle-ear space
- Perforation
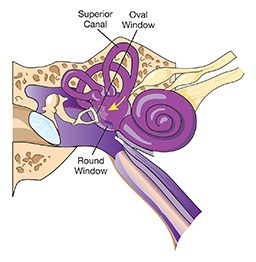
Inner-Ear Barotrauma
Inner-ear barotrauma is damage to the inner ear due to pressure differences caused by incomplete or forceful equalization. A leak of inner-ear fluid may or may not occur.
Mechanisms of injury
The inner ear is separated from the external world by the middle ear. It is the organ for hearing and balance. When the pressure in the middle-ear space is properly equalized, the risk of inner-ear barotrauma is extremely low.
If the pressure in the middle ear is not equalized during descent, the water pressure on the eardrum transfers inward through the middle-ear ossicles to the oval windows, and the round window bulges outward. The pressure itself may damage sensitive inner-ear structures. If the pressure is excessive, either the oval window or, more commonly, the round window may tear, and the inner-ear fluid (perilymph) may leak into the middle ear (perilymph fistula).
The Valsalva maneuver increases the pressures in cranial tissues and circulation, which may transmit to the cochlear fluid, causing an outward movement of the round window. Pressure waves alone can cause damage to the inner ear without window rupture. If the rupture occurs, the loss of fluid from inner ear leads to damage of the hearing organ and sometimes of the balance organ. If the leak is not stopped soon by spontaneous healing or surgical repair, permanent hearing loss may occur.
Manifestations
Divers may experience:
- Severe vertigo
- Hearing loss
- Ears roaring/ringing (tinnitus)
- Involuntary eye movement (nystagmus)
- Fullness of the affected ear
Symptoms of middle-ear barotrauma are almost always present. Vertigo is usually severe and accompanied by nausea and vomiting. Hearing loss can be complete, instant and permanent, but divers usually lose just the higher frequencies. The loss becomes noticeable only after a few hours. You may not be aware of the loss until you have a hearing test.
Management
In case of vertigo underwater, abort the dive, and obtain assistance to reach the surface safely. Begin surface oxygen if decompression illness is suspected. First aid providers should conduct a complete neurological exam and note any deficits.
Inner-Ear Barotrauma or Inner-Ear Decompression Sickness?
It is important to distinguish between these two conditons, because their treatments differ. The standard treatment for DCS of any kind is hyperbaric oxygen treatment in a recompression chamber; recompression or any pressure change is contraindicated when inner-ear barotrauma is likely. While the symptoms are similar in both conditions, barotrauma is preceded by failed equalization of middle-ear pressure and usually occurs at the beginning of dive, while DCS occurs due to failed decompression at the end of the dive.
Definitive Treatment
Urgently seek an evaluation by a physician to rule out DCS. If your physician determines it is not DCS, consult an ENT specialist with experience treating divers. For a referral in your area, email , or call the DAN Medical Information Line at +1 (919) 684-2948.
Avoid any exertion, middle-ear equalization, altitude or diving exposure, sneezing or nose blowing. Do not take aspirin, nicotinic acid (vitamins), other vasodilators or anticoagulants. Conservative treatment includes bed rest in a sitting position and avoiding any strains that can increase intracranial or middle-ear pressure. If symptoms do not improve, surgery may be necessary. Healing of the tear (fistula) usually occurs within a week or two. Hearing loss may become permanent.
Fitness to Dive
Evaluation of fitness to dive requires an expert diving physician and depends on the degree of permanent damage as well as the probability of repeated injury.
Prognosis
In many cases, complete healing occurs spontaneously. If fistula presents and does not heal soon spontaneously, surgery may be recommended. In some cases, the inner ear may be damaged permanently; the body may adapt to one side not working properly. If injury occurs to the other ear, the situation can be serious and may involve incapacitating balance problems.
Prevention
Learn gentle but effective equalization techniques, and avoid aggressive employment of the Valsalva maneuver. Do not dive when congested.
Perilymph Fistula
A perilymph fistula is a tear in the round- and/or oval-window membranes through which inner-ear fluid (perilymph) is leaking.
Mechanism
Leakage of perilymph from the labyrinth may occur when the round or oval window is disrupted due to severe middle-ear barotrauma or forceful Valsalva maneuver.
Manifestations
The symptoms of perilymph fistula may include dizziness, vertigo, imbalance, nausea and vomiting. Some people experience ringing (tinnitus) and fullness in the ears, and many notice some hearing loss. Symptoms worsen with changes in altitude (elevators, airplanes or travel over mountains), weather changes and with physical exertion.
Management
This condition can usually be managed conservatively with absolute bed rest in the sitting position. Straining, sneezing, nose blowing, sexual activity, loud noises and middle-ear equalizing should be avoided to prevent pressure waves in the inner ear.
The round-window fistula often heals spontaneously within a week or two with this regimen, but if hearing loss progresses or the other features persist, it may be necessary to resort to surgery to repair the round-window leak.
Fitness to Dive
Even after the acute symptoms of an oval- or round-window fistula have resolved, the diver’s future in diving is questionable. Flying should be completely avoided for several months to allow complete healing of the injury or the surgical repair.
For a referral in your area, email , or call the DAN Medical Information Line at +1 (919) 684-2948.
Prevention
Ensure the Eustachian tubes are functioning properly before diving by gently equalizing on the surface.
Alternobaric Vertigo
Alternobaric vertigo occurs during descent, ascent or immediately after surfacing from a dive and is caused by unequal pressure stimulation in each ear.
Statistics
According to various sources, up to 25 percent of divers experience alternobaric vertigo at some time.
Mechanisms
During ascent, air in the middle-ear space expands, relative pressure increases, the Eustachian tubes open passively, and gas escapes through the Eustachian tubes into the nasopharynx. Occasionally the Eustachian tube may obstruct this flow of air, with subsequent air distension and increased pressure sensation in the middle-ear cavity during ascent. If the obstruction is one-sided and the pressure difference is greater than 60 centimeters of water, vertigo may occur as the pressure increase stimulates the vestibular apparatus. Usually it is relieved by further ascent, because the increasing differential pressure in the middle-ear space forces open the Eustachian tube and vents the excess air. Contributing factors include middle-ear barotrauma during descent, allergies, upper respiratory infections (congestion) and smoking.
Manifestations
The symptoms of alternobaric vertigo may include disorientation, nausea and vomiting.
Note: The disorienting effects of vertigo while diving are extremely dangerous. The inability to discern up from down, follow safe ascent procedures, and the risks associated with vomiting pose a significant hazard to the diver as well as other divers in the water.
Management
Advice provided by Dr. Carl Edmonds about how to manage alternobaric vertigo during a dive:
“If a diver encounters ear pain or vertigo during ascent, he should descend a little to minimize the pressure imbalance and attempt to open the Eustachian tube by holding the nose and swallowing (Toynbee or other equalization maneuver). If successful, this equalizes the middle ear by opening it up to the throat and relieves the distension in the affected middle ear.
“Occluding the external ear by pressing in the tragus (the small fold of cartilage in front of the ear canal) and suddenly pressing the enclosed water inward may occasionally force open the Eustachian tube. If this fails, then try any of the other techniques of equalization described previously, and attempt a slow ascent.”
Uncomplicated cases resolve quickly within minutes upon surfacing. If symptoms persist, see your primary care physician or an ENT specialist. Do not dive if you have equalization problems.
Associated injuries include middle-ear barotrauma and inner-ear barotrauma; alternobaric vertigo may occur during descent or ascent, but is commonly associated with a middle-ear barotrauma of ascent (reverse squeeze). Other conditions such as inner-ear DCS or caloric vertigo (when cold water suddenly enters one ear) should be ruled out.
Fitness to Dive
As soon as all symptoms and contributing factors have been resolved, a diver may return to diving.
Prevention
Take measures for the prevention of ear barotraumas. Avoid the unequal pressurization of the ear by avoiding tight-fitting wetsuit hoods or earplugs. Maintain good aural hygiene. Do not dive when congested or unable to equalize.
Reverse Squeeze
A reverse squeeze is barotrauma due to an inability to release pressure from the middle ear on ascent.
Mechanisms
Pressure must be released from the middle ear as the diver ascends, or the expanding air will bulge and even rupture the eardrum. Expanding air normally escapes down the Eustachian tubes, but if the tubes are blocked with mucus at depth (usually the result of poor equalization on descent, diving while congested or relying on decongestants that wear off at depth), barotrauma can result.
Manifestations
- Pressure, fullness in ear
- Ear pain
- Vertigo
Management
While diving: Sometimes one of the equalizing techniques used on descent will clear your ears on ascent. Pointing the affected ear toward the bottom may help, too. Ascend as slowly as your air supply allows. Increasing pressure usually opens the Eustachian tube and relieves overpressure. However, in rare cases it may persist all the way up. In that case, you will have to endure the pain to reach the surface. Notify your buddy, and stay in close proximity.
First aid: Nasal decongestant spray may help open the Eustachian tube. A physician evaluation is advised if you experience vertigo, protracted pain and fullness of the ears.
Fitness to Dive
Repeated episodes require an ENT evaluation. For an ENT referral in your area, email , or call the DAN Medical Information Line at +1 (919) 684-2948.
Prevention
Prior to diving, try equalizing on the surface to ensure Eustachian tube function is adequate.
Facial Baroparesis
Facial baroparesis is reversible paralysis of the facial nerve due to increased pressure in the middle ear when ascending in an airplane or from scuba diving.
Mechanisms

The facial nerve is a cranial nerve that controls the muscles of the face. On its way from the muscle to the brain it passes through the channel in the wall of the middle-ear space. Pressure changes in that space normally have little or no effect on the nerve.
In some people, the canal of facial nerve misses the bony wall and is separated from the middle-ear cavity by only a thin membrane. If such a person experiences an overpressure in the middle ear equal or greater to the capillary pressure, circulation to the facial nerve stops, the facial nerve loses its functionality and facial muscle is paralyzed (facial baroparesis). This can happen while flying or diving. Fortunately, the pressure in the middle ear returns to normal soon after the exposure, restoring the circulation to the nerve and enabling its functionality. Facial baroparesis tends to recur with flying or repeated diving.
Manifestations
Symptoms include numbness, paresthesia, weakness or even paralysis of the face. Decreased sensation and a facial droop can be seen, generally on one side of the face.
Management
Facial baroparesis usually is discovered postdive. Even when its duration is brief and it resolves spontaneously, the patient should be evaluated by a physician to exclude other possible causes such as stroke, infection, trauma or decompression sickness.
In rare instances of protracted facial baroparesis, treatment may be necessary. There is experimental evidence that overpressure lasting more than 3.5 hours may cause permanent damage. Divers who continue to experience facial numbness and drooping should see a physician within three hours.
Fitness to Dive
This condition is self-limiting and resolves spontaneously within hours, but it can recur with diving or flying. Return to diving may be considered when symptoms have completely resolved and have been determined to be the result of facial barotrauma.
Prevention
Learn gentle but effective equalization techniques. Do not dive with congestion.
Temporomandibular Joint Syndrome (TMJ)
Temporamandibular joint syndrome is pain in and around the temporomandibular joint caused by prolonged gripping of a mouthpiece from a snorkel or scuba regulator.

Statistics
It has been reported that TMJ occurs in 15-20 percent of snorkelers and scuba divers.
Mechanism
TMJ is a chronic inflammation of the jaw joint just in front of the ear. The pain can be great enough to make holding the mouthpiece between the teeth difficult. The condition is exacerbated by local factors such as joint laxity, anatomical factors, capsular or muscular inflammation, or the type of mouthpiece used.
Diving-associated TMJ is thought to result from the forward posturing of the mandible by an ill-fitting mouthpiece and clenching of the mouthpiece, especially with heavy regulators. Diving may aggravate preexisting TMJ. The pain is sometimes severe enough to cause divers to abort the dive. It can occur in novice divers who clench their teeth, sometimes with such intensity that they occasionally bite through the mouthpiece.
Manifestations
- Pain in the TMJ and ears
- TMJ clicking or crepitus (cracking or popping sound)
- Trismus (inability to open mouth fully) and impaired TMJ mobility
- Dizzy spells (could be hazardous should it occur underwater)
- Masticatory muscle pain
- Stuffy sensation in the ears
- Eustachian tube dysfunction
- Headache and facial pain
Management
While diving: Work to relax your bite while retaining the mouthpiece in place. If unsuccessful, safely end the dive, surface and consider alternative mouthpiece options.
Definitive treatment: If pain persists, a consultation with a specialist is suggested as solutions are highly individualized. Treatment includes bite adjustment, management of dental problems and the use of orthodontic mouthpieces. Heat and anti-inflammatory drugs are helpful.
Fitness to Dive
Return to diving is possible upon pain resolution. You must also be able to grip the mouthpiece without pain.
Prevention
Use only a mouthpiece that fits properly. Consider a customized mouthpiece. Correct contributing conditions such as dental problems, anxiety and teeth grinding (bruxism).
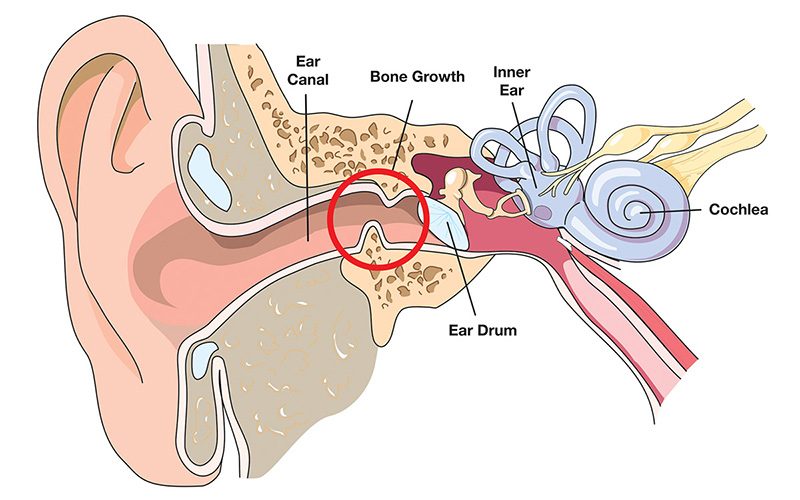
Surfer’s Ear
Surfer’s ear is the narrowing of the outer ear canal due to an abnormal growth of bone caused by exposure to cold and wet conditions.
Mechanism
The external ear canal is a tubular structure that conducts sounds and protects the middle ear. Exostosis is a chronic condition characterized by narrowing of the inner half of the ear canal as a result of bone growth. The bony wall grows outward slowly over a period of years in response to local irritation by cold water. These growths are called swimmer’s nodes and are common in swimmers, surfers and divers. This condition is not related to infection nor is it caused by infection; however, the narrowing of the ear canal may prevent water from draining out, which increases susceptibility to outer-ear infections. The bony swellings continue to grow while there is a continued exposure to cold water (such as that found in seawater and outdoor swimming pools in temperate climates). Exostosis often occurs in outdoor enthusiasts in their mid- to late-30s, but individuals who experience significant cold-water exposure — such as surfers, swimmers and divers — can develop the condition earlier.
The narrowed ear canal is more prone to blockage by earwax or debris and more susceptible to swimmer’s ear (otitis externa). An exostosis on the floor of the ear canal can form a sump that retains moisture and is susceptible to infection. Exostosis is seen as a narrowing of the ear canal. The average ear canal is about 0.25 inches wide (7 milimeters). The bone growth may cause it to narrow to 0.04 inches (1 millimeter). Early signs include water trapping in the ear canal after swimming. Debris trapping and infections may make surgery necessary.
Manifestations
External ear infections and difficulty removing water from the external ear canal may be recurrent. Exostosis symptoms in advanced cases include a decreased hearing possibly combined with an increased prevalence of ear infections.
Differential Diagnosis
Other causes of external ear-canal obstruction could include infection or earwax (cerumen) impaction.
Treatment
In case of decreased hearing or repeated infections, exostosis may be removed surgically.
Fitness to Dive
Exostoses do not affect fitness to dive unless they are occluding the ear canal or causing recurrent infection.
Prevention
- Wear a hood in cold water.
- After diving, rinse both ears with freshwater to flush contaminated water and salt.
- If prone to ear infections, blow warm air into external canal using a hair dryer (take care to make sure the air is not too hot).
- If your ears have a natural tendency to build up a blockage of earwax, have them checked regularly, particularly before a prolonged diving trip.
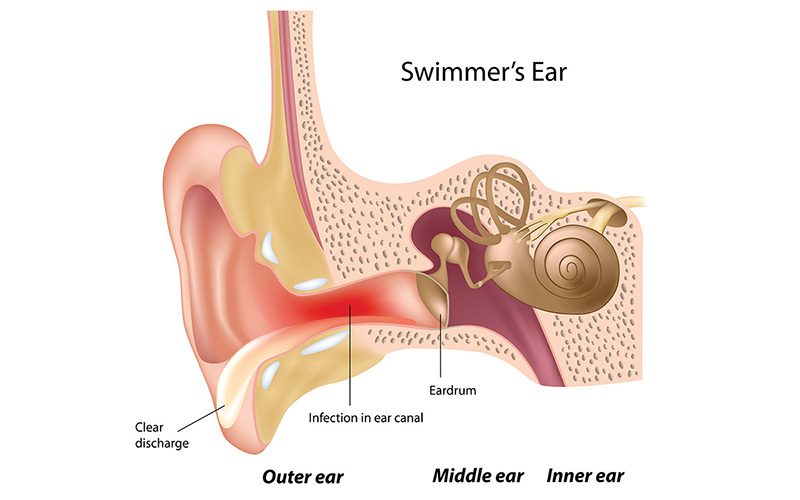
Swimmer’s Ear
Acute inflammation or infection of the outer ear (pinna and ear canal) caused by prolonged exposure to wet and warm conditions is known as swimmer’s ear.
Statistics
Otitis externa affects one in 200 Americans every year and is present in chronic form in 3-5 percent of the population. Swimmers, surfers and other individuals who are exposed to wet and warm conditions are at an increased risk.
Mechanism
The external auditory canal is the tubular opening between the outside environment and the eardrum (tympanic membrane). It is covered by skin and secretes earwax (cerumen), which helps protect against infection.
Otitis externa, commonly referred to as swimmer’s ear, is the acute inflammation or infection of the external auditory canal, resulting in ear pain and pus discharge.
Breakdown of the external ear canal’s protective barrier leads to infection. Excessive moisture, mechanical trauma or underlying skin conditions are contributing factors. The bacteria normally found in the external ear canal often trigger the infection. With frequent immersion, water swells the cells lining the ear canal. Eventually, these cells separate far enough for the bacteria that are normally found on the surface of the ear canal to penetrate the skin, where they find a warm environment and start to multiply. Otitis externa is more likely to develop if the skin in the ear canal is already chafed and cracked by excessive moisture from showering or scratching. Bacteria or fungus from the water can easily invade damaged skin.
Seborrheic dermatitis, psoriasis and excessive cleaning of wax from the ears that injures the skin lining the external ear canal may increase susceptibility of the ear canal to infection. Excessive debris or cerumen may trap water in the canal.
Manifestation
The chief complaint is generally itching often accompanied by pain, tenderness and swelling of the ear canal. If left untreated, the swelling can increase to include nearby lymph nodes and produce enough pain that moving the jaw becomes uncomfortable.
Management
First Aid
- Avoid getting in the water until after the problem clears up.
- Use a hair dryer to carefully dry the ear after you shower (take care to ensure the air is not too hot).
- In case of pain, over-the-counter pain medications can be effective. Examples of such medications include acetaminophen (Tylenol), ibuprofen (Advil or Motrin) or naproxen (Aleve). Read and follow all instructions on the label.
Treatment
Stop swimming and diving; schedule an appointment with your physician. Do not put anything in your ear unless instructed to do so. If you have diabetes or take medicine that suppresses your immune system, swimmer’s ear can cause severe problems that require immediate medical attention.
It is important for your physician to rule out external ear squeeze, otitis media and mastoiditis (infection of the bone just behind the ear).
Fitness to Dive
Return to diving is possible once your physician determines that the infection
has resolved.
Prevention
Keep your ears clean and dry.
- Dry ears with a towel after swimming or showering by tilting your head and pulling your earlobe in different directions while your ear is facing down.
- Refrain from putting objects — such as cotton swabs or your finger — in the ear canal or removing ear wax yourself; both actions can damage the skin, potentially increasing the risk of infection.
- You can dry your ears with a blow dryer if you put it on the lowest setting and hold it at least a foot (about 0.3 meters) away from the ear.
- Talk to your doctor about whether you should use alcohol-based eardrops after swimming.
If you know you don’t have a punctured eardrum, you can use over-the-counter eardrops or homemade preventive eardrops before and after swimming. This mixture of one part white vinegar to one part rubbing alcohol may help promote drying and prevent the growth of bacteria and fungi that can cause swimmer’s ear. At the end of each day of diving, put five drops of the solution into each ear. Let it stay for five minutes before draining back out.
Next: Chapter 3 – Symptoms >