Middle-ear barotrauma (ear squeeze) is the most common dive injury. It occurs when pressure in the air space of the middle ear is not equalized to the ambient pressure. It can cause a ruptured eardrum and can happen either while diving or flying.
Anatomy and Functions of the Ear
The human ear has three distinct sections:
- External ear: This includes the ear itself and the ear canal to the eardrum.
- Middle ear: This is an air-filled cavity between the eardrum and the inner ear. It has three components: the middle-ear cavity, the three ear bones (ossicles) and the mastoid process.
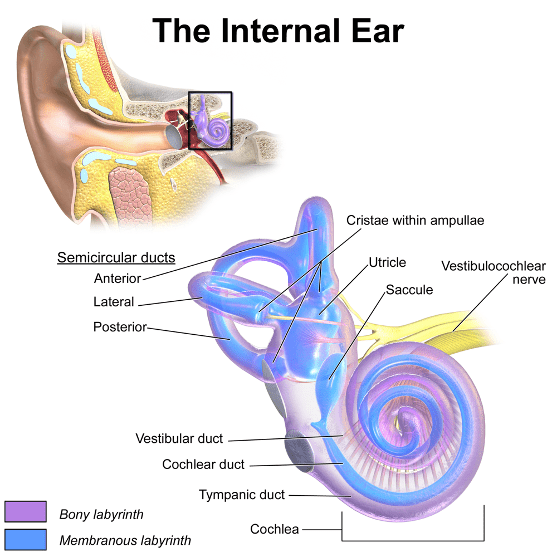
- Inner ear: The inner ear is a sensory organ. It is part of the central nervous system, and it has two functions:
- Auditory: The cochlea turns soundwaves into electrical impulses for the brain.
- Balance, orientation and acceleration: The canals provide some of our control of balance and position and help detect acceleration.
Mechanisms of Injury
The air pressure in the tympanic cavity — an air-filled space in the middle ear — must be equalized with the pressure of the surrounding environment. The Eustachian tube connects the throat with the tympanic cavity and provides passage for gas when pressure equalization is needed. This equalization normally occurs with little or no effort. Various maneuvers, such as swallowing or yawning, can facilitate the process.
An obstruction in the Eustachian tube can lead to an inability to achieve equalization, particularly during descent, when the pressure changes quickly. If the pressure in the tympanic cavity is lower than the pressure of the surrounding tissue, this imbalance results in negative pressure (a relative vacuum) in the middle-ear space. It causes tissue to swell, the eardrum to bulge inward, leakage of fluid and bleeding of ruptured vessels. At a certain point an active attempt to equalize will be futile, and a forceful Valsalva maneuver may injure the inner ear. Eventually the eardrum may rupture; this is likely to bring relief from the pain associated with MEBT, but it is an outcome to avoid if possible.
Often the injury is serious enough that it causes rupture of the eardrum, tympanic membrane rupture or inner ear barotrauma.
Factors that can contribute to the development of MEBT include the common cold, allergies or inflammation — conditions that can cause swelling and may block the Eustachian tubes. Poor equalization techniques or too rapid descent may also contribute to the development of MEBT.
Manifestations
Divers who cannot equalize middle-ear pressure during descent will first feel discomfort in their ears (clogged or stuffed ears) that may progress to severe pain. Further descent only intensifies the ear pain, which is soon followed by a serous fluid buildup and bleeding in the middle ear. With further descent, the eardrum may rupture, providing pain relief; this rupture may cause vertigo and hearing loss. Exposure of the normally sterile middle ear to infection from a mixture of pathogens from the non-sterile contents of the ear canal and surrounding water may result in a middle-ear infection.
Signs and Symptoms
- A feeling of clogged or stuffed ears
- Ear discomfort or pain
- Pain increases with descent during diving
- Fluid buildup and bleeding
- Eardrum rupture, leading to vertigo and hearing loss
Prevention
- Do not dive when congested.
- Refrain from diving when feeling popping or crackling in your ears, or if you have a feeling of fullness in your ears after diving.
- Learn and use proper equalization techniques.
First Aid
- Use a nasal decongestant spray or drops. This might reduce the swelling of the mucous membranes, which may help to open the Eustachian tubes and drain the fluid from the middle ear.
- Do not put any drops in your ear canal. If the tympanic membrane is ruptured, this might make things worse.
- Seek professional medical evaluation. Any doctor should be able to help, regardless of any dive medicine knowledge or training.
Implications for Diving
For the Diver
- You can consider a return to diving if a physician determines that the injury has healed, and the Eustachian tube is functional.
- Do not neglect these injuries. Some of the complications could negatively affect you for the rest of your life.
- Return to your physician if you have worsening pain, fever or discharge. These may indicate a middle-ear infection.
For the Dive Operator
- Have the diver evaluated by a medical professional in a timely fashion.
- Don’t worry about referring them to a doctor with dive medicine experience. An ear, nose and throat (ENT) doctor (otolaryngologist) is ideal for both ear and sinus problems, but your primary care physician can help for most common problems.
For the Physician
- Provide symptomatic treatment (anti-inflammatory drugs, decongestants, mucolytic agents).
- Prophylactic antibiotic therapy is controversial. Although a middle-ear infection is a plausible secondary complication, this is not always the case in the acute phase.
- Assess tympanic membrane perforation (this is sometimes difficult to recognize).
- If present, consider referring the patient to an ENT specialist.
- Use the O’Neill grading system or detail what you observe.
- Assess the vestibular function.
- Vertigo, nystagmus and/or hearing loss might be suggestive of inner-ear barotrauma. If present, strongly discourage your patient from further diving until properly cleared by a specialist.
Fitness to dive
Do not dive until swelling and inflammation have resolved, and you can adequately equalize, preferably under otoscopic evaluation. Assess why the problem occurred (lack of training, allergy, etc.) and address each factor. If you are unable to equalize, then you may consider ENT consultation. The inability to equalize properly is disqualifying.
Note: Do not dive with earplugs, as this may cause external-ear barotrauma.