Never stop developing your diving abilities. There is always more to learn—how to dive new environments, how to refine your skills or even how to use new types of equipment. No matter where your diving adventures take you, make sure you are equipped with the proper training.
Remember:
Your certification only qualifies you for the same diving conditions and the environment in which you were trained.
As you continue your training, slowly extend your diving experiences. California shore diving presents different challenges than Caribbean boat diving—make sure you’re prepared for each new diving environment.
Take it easy, and if you’re not having fun or if you don’t feel good about the dive, don’t do it. This is especially important when diving in new conditions such as cold water or limited visibility or when using new equipment.
If you feel uncomfortable about a dive, it may because you feel that you’re not ready. Remember, dive your experience, not your “C” card.
If you want to begin exploring new environments, seek the proper training that will prepare you to explore them safely. For instance, if you want to explore the interiors of shipwrecks or enter a cave, enroll in a Wreck Diving or Cave Diving course. These unique overhead environments present specific challenges that can be deadly if you are not trained to manage them.
Don’t neglect first aid training. In the case of an emergency, you will not regret taking a course that requires a few hours of your time.
There are all kinds of specialty dive courses that can prepare you to explore safely. If you want to expand your diving experiences, sign up for a course to get the training you need…
Running out of air is the most common trigger for diving accidents. It seems like a no-brainer, but several factors can affect consumption rate. Be air aware: Monitor your air supply.
Incorporate gas supply into your dive planning. You can only stay under as long as you have enough gas remaining for a safe ascent. Don’t forget to save some gas for flotation. Good rules of thumb for turnaround limits are when you have used:
Check your gauge regularly.
Be aware that exertion, like when swimming in strong currents and depth will affect your air consumption.
Anxiety or stress can also affect air consumption. Try to maintain normal breathing, but if you do feel anxious, keep a closer eye on your gas supplies; it may dwindle more rapidly than usual.
Running out of air is an easily avoidable mistake that carries serious repercussions.
Each diver in the dive group shares equal responsibility for the conduct of the dive. When all divers understand and agree with that premise, the dive group can protect itself from individual and collective harm.
Know your personal limits and take time to examine and evaluate your dive habits.
Don’t rely on the experience of other divers in the group. As a certified diver, you are expected to recognize when elements are outside your level of training or comfort zone; it is your responsibility to acknowledge that and voice it.
Always remember, anyone can call off a dive at any time. In other words, it’s always OK to say “No.”
DIVE SAFETY STARTS WITH YOU.
13 Ways to Run Out of Air & How Not To
DAN’s Smart Guide to Air Consumption
Our self-contained underwater breathing apparatuses are only useful as long as the tank contains sufficient breathing gas. Scuba equipment allows us to breathe underwater, extending our ability to explore. Without breathing gas, our time is limited by the dangers of asphyxia and drowning.
During dive training you learned how to:
Understand breathing gas needs
Calculate the limits of available gas
Monitor the remaining gas pressure
Return to the surface in a timely manner with enough gas to inflate your BCD
Even so, running out of breathing gas is the most common dive incident and the number one cause of diving fatalities. Even the most skilled divers can make mistakes and run out of gas. In this guide, we’ll cover the 13 most common errors that lead to out-of-air emergencies and how to avoid these situations.
Gas consumption increases dramatically with depth. Your decompression obligation builds quickly, and you may need more gas for decompression stops. An Aluminum 80 is not meant for deco dives. Running out of gas at depth puts you at risk of a long, hazardous emergency ascent. You can maximize your time at shallower depths and easily reach the surface in the event of an emergency.
2. Staying Too Long
Sooner or later you will consume your gas reserves. Determine in advance the tank pressure at which you will need to turn back and start your ascent. During the dive, actively monitor your tank pressure and turn back on time.
3. Working too Hard
Fighting a strong current, hunting or lacking buoyancy control can affect air consumption. Exertion at depth may speed up depletion of your tank up to twenty times. If you are not accustomed to diving in strong currents or surf, seek training prior to diving in these environments.
4. Not Monitoring Your Pressure Gauge
Be air aware: Monitor your air supply. Check your pressure gauge regularly and communicate your supplies with your buddy.
5. Ignoring Anxiety as a Factor
Anxiety changes all calculations and may deplete tank reserves faster than vigorous exercise. Try to maintain normal breathing, but if you do feel anxious, keep a closer eye on your gas supplies; it may dwindle more rapidly than usual.
Procedural Problems
6. Starting With Less Than a Full Tank
Regardless of how short an immersion you may contemplate, do not start your dive on less than a full tank. Never descend to retrieve a lost piece of equipment or anchor if the tank is nearly empty.
7. Not Opening the Tank Valve All the Way
Open the tank valve all the way and check that breathing through the regulator does not cause the pressure indicator to swing with each breath
8. Frequent Depth Changes and BCD Adjustments
Yo-yo diving, or using your BCD frequently to move up and down in the water column, can quickly deplete your gas supply. Yo-yo diving also increases risk of pulmonary barotrauma and decompression sickness.
9. Omitting Predive Check and Buddy Checks
Use a printed predive checklist to prevent mental lapses—the mental checklist is an oxymoron.
Equipment Issues
10. Regulator
Your gas consumption can be affected if:
Your regulator is hard to breathe from.
Your regulator starts to free-flow due to freezing or debris.
Your dive buddy accidentally knocks your regulator out of your mouth.
Your secondary regulator has a slow leak.
Your mouthpiece decouples from your regulator.
Take preventive steps:
Rinse your regulator after diving.
Conduct regular maintenance on your regulator and have all parts replaced that may have been worn off or are out of date.
Secure your spare regulator—don’t let it drag on the bottom.
If your regulator starts to free flow, attempt to flush it; this may help if debris is to blame. Remember, you can still breathe from a free-flowing regulator, but the gas will not last long, so you have to initiate the ascent.
11. BCD
Inflator leaks or tears in your BCD can deplete your air. Rinse your BCD after diving and conduct regular maintenance to prevent leaks.
12. Pressure Gauge
If your pressure gauge is integrated with your computer, a computer error may also affect the gauge. If your tank pressure does not decrease with time of dive, you have a problem and should safely terminate the dive. Make sure that your gauge is calibrated properly. Some gauges will not indicate zero, even when the tank is empty. To avoid this problem, make sure you return to the surface with the gauge indicating 500 psi or greater.
13. Burst O-ring or Hose
O-rings should be replaced regularly. Carry your own with you, and if you have a minor leak, replace the O-ring in question. Do not open your regulator on your own; this should only be done by a certified maintenance professional.
Your breathing rate depends on your level of exercise and depth. The higher your level of exercise, the more oxygen you need and the more CO2 you will produce. In order to flush the CO2 from your lungs while diving, you must inhale breathing gas. The chart below shows the relationship between depth, pressure, exercise and breathing gas requirements. The deeper the depth and the higher the level of exercise, the greater the demand for breathing gas.
Breathing Gas Needs: How Much Air is Required to Ventilate Lungs?
Depth (Feet)
Environmental Pressure (Atmospheres)
Breathing gas Needs (Liters per minute)
At rest
Light to moderate activity
Vigorous exercise
0 feet (Surface)
1 ATM
8 lpm
20 lpm
70 lpm
30 feet
2 ATM
16 lpm
40 lpm
140 lpm
100 feet
4 ATM
32 lpm
80 lpm
280 lpm
By the Numbers
The Aluminum 80 is the most commonly used tank.
Specifications:
Internal tank volume: 11 liters (0.39 cubic feet).
1 Maintain your equipment regularly and inspect any rental equipment carefully.
2 Use a written predive checklist and plan the maximum depth and duration of your dive that can be safely achieved with the available supply.
3 Open the tank valve all the way. (Consider buying a tank with an open/close valve indicator.)
4 Conduct a predive test breath on your regulator and make sure your tank is full before the dive. Also, check the gas line and complete an in-water buddy check before descending.
5 Carry an independent emergency gas reserve. Two independent gas sources are better than one. It may help you in your own emergency or if another diver requests your breathing gas.
6 Monitor your tank pressure at regular intervals.
7 Stay within your dive training limits.
8 Turn back when you exhaust half of your available gas supply and make sure you conserve enough air for flotation on the surface.
Before the Dive
Turn Back
Bring to the Surface
3000 psi
1500 psi
500 psi
9 Adjust your buoyancy in protected, shallow water. If you find you have buoyancy problems, abort the dive and fix the problem.
Safety Starts With You
This is an easily avoidable mistake that can carry serious repercussions. The best strategy is not to run out of gas. If you run out of your gas toward the end of dive, your buddies are probably also low on gas and there may not be enough supply to manage two stressed divers. Monitoring your gas supply is a simple step to preventing a serious situation. Dive safely.
Hazardous Marine Life
While exciting, observing marine life in their environment comes with a risk. Injuries, though rare, may occur as a result of an uninformed swimmer or diver’s actions. The Hazardous Marine Life reference book examines the most common hazardous marine life that water enthusiasts may encounter and introduces the mechanisms of injury, techniques for injury prevention and application of first aid.
Envenomation is a process by which a venom or toxin is injected into another being via a bite, puncture or sting. Envenomation is always due to direct contact with an animal (or parts of it like drifting jellyfish tentacles). There are two possible mechanisms of injection: active, such as jellyfish or cone snails, or passive like lionfish or sea urchins. Injuries typically occur during shore entries or exits, incidental contact or deliberate attempts to handle a specimen. Envenomations are rare but can be life-threatening and may require rapid first aid response. In this chapter, we will cover some common envenomations as well as some of the more rare, but serious cases.
Fire corals are colonial marine cnidarians that when touched can cause burning skin reactions. Fire coral-related incidents are common among divers with poor buoyancy control.
Biology and Identification
Fire coral, which belong to the genus Millepora, are found in tropical and subtropical waters around the world. Generally fire coral adopts a yellow-green or brownish branchy formation, although its external appearance often varies due to environmental factors. Because fire coral can colonize hard structures, it can even adopt a rather stony appearance with rusty coloration.
Despite their calcareous structure, fire coral is not a true coral; these animals are more closely related to Portuguese man-of-war and other hydrozoans.
Mechanism of Injury
Fire coral gets its name because of the fiery sensation experienced after coming into contact with a member of the species. The mild to moderate burning that it causes is the result of cnydocites embedded in its calcareous skeleton; these cnydocites contain nematocysts that will fire when touched, injecting their venom.
Signs and Symptoms
The burning sensation may last several hours and is often associated with a skin rash that appears minutes to hours after contact. This skin rash can take several days to resolve. Often, the skin reaction will subside in a day or two, but it may likely reappear several days or weeks after the initial rash disappeared.
Fire coral lacerations, in which an open wound receives internal envenomation, are the most problematic fire coral injuries. Venom from Millepora spp. is known to cause tissue necrosis on the edges of a wound. These injuries should be carefully observed, as necrotic tissue provides a perfect environment to culture serious soft tissue infections.
Fire coral are found in tropical and subtropical waters around the world.
Prevention
Avoid touching these calcareous formations.
If you need to kneel on the bottom, look for clear sandy areas.
Remember that hard surfaces such as rocks and old conchs may be colonized by fire coral even if they do not look branchy.
Always wear full-body wetsuits to provide protection against the effects of contact.
Master buoyancy control.
Always look down while descending.
First Aid
Rinse the affected area with household vinegar.
Redness and vesicles will likely develop. Do not puncture them; just let them dry out naturally.
Keep the area clean, dry and aerated—time will do the rest.
For open wounds, seek a medical evaluation. NOTE: Fire coral venom is known to have dermonecrotic effects. Share this information with your physician before any attempts to suture the wound, as the wound edges might become necrotic.
Antibiotics and a tetanus booster may be necessary
Portuguese Man-of-War
Portuguese man-of-wars are free-floating cnidarians characterized by blue gas-filled bladders and long tentacles that drift on the surface of the ocean. Contact with a man-of-war’s tentacles can cause intense pain and other systemic symptoms.
Biology and Identification
There are two species for the genus: Physalia physalis in the Atlantic and Physalia utriculus in the Indo-Pacific. The Atlantic man-of-war may reach slightly larger dimensions, with the gas bladder rarely exceeding one foot (30 centimeters) and tentacles averaging 33 feet (10 meters) and possibly extending up to 165 feet (50 meters).
Though many people mistake the Portuguese man-of-war for species of jellyfish, this genus belongs to the order Siphonophora, a class of hydrozoans. What we see as a single specimen is actually a colony composed of up to four different types of polyps. Despite its resemblance, these animals are more closely related to fire coral than to jellyfish.
The Portuguese man-of-war is easily recognizable; if you see blue tentacles, you can bet they belong to Physalia.
Risk to Humans
The man-of-war’s polyps contain cnidocytes delivering a potent proteic neurotoxin capable of paralyzing small fish. For humans, most stings cause red welts accompanied by swelling and moderate to severe pain. These local symptoms last for two to three days.
Systemic symptoms are less frequent, but potentially severe. They may include generalized malaise, vomiting, fever, elevated heart rate at rest (tachycardia), shortness of breath and muscular cramps in the abdomen and back. Severe allergic reactions to the man-of-war’s venom may interfere with cardiac and respiratory function, so divers should always seek a timely professional medical evaluation.
Epidemiology
Approximately 10,000 cnidaria envenomations occur each summer off the coasts of Australia, the vast majority of which involve Physalia. In fact, man-of-wars cause the most cnidarian envenomations prompting emergency evaluation globally. The risk may not be so great for divers, however, as most Physalia stings occur on beaches or on the surface of the water rather than while submerged. Certain regions are known to have seasonal outbreaks, but incidence is highly variable between regions.
Prevention
Always look up and around while surfacing. Pay special attention during the last 15-20 feet of your ascent, since this is the area where you may find cnidarians and their submerged tentacles.
Wear full body wetsuits regardless of water temperature. Mechanical protection is the best way to prevent stings and rashes.
In areas where these animals are known to be endemic, a hooded vest may be the best way to protect your neck.
First Aid
Avoid rubbing the area. Cnidarian tentacles are like nematocyst-coated spaghetti, so rubbing the area or allowing the tentacles to roll over the skin will exponentially increase the affected surface area and, therefore, the envenomation process. NOTE: Initial pain may be intense. Though life-threatening complications are rare, monitor circulation, airway and breathing, and be prepared to perform CPR if necessary.
Remove the tentacles. You must take great care to remove the man-of-war’s tentacles in order to avoid further envenomation. Those distinctive blue tentacles are quite resistant to traction, so you can remove them fairly easily with some tweezers or gloves. NOTE: If you do not have access to tweezers or gloves, the skin on your fingers is likely thick enough to protect you. Keep in mind, however, that after removal your fingers may contain hundreds or even thousands of unfired nematocysts, so pretend you have been handling hot chili peppers that cause blisters anywhere you touch and treat your fingers as recommended from the next step on.
Flush the area with seawater. Once the tentacles and any remnants have been removed, use a high volume syringe and flush the area with a powerful stream of seawater to remove any remaining unfired nematocysts. Never use freshwater since this will cause unfired nematocysts to fire.
Apply heat. Immerse the affected area in hot water (upper limit of 113°F/45°C) for 30 to 90 minutes. If you are assisting a sting victim, try the water on yourself first to assess tolerable heat levels. Do not rely on the victim’s assessment, as intense pain may impair his ability to evaluate tolerable heat levels. If you cannot measure water temperature, a good rule of thumb is to use the hottest water you can tolerate without scalding. Note that different body areas have different tolerance to heat, so test the water on the same area where the diver was injured. Repeat if necessary. If hot water is not available, apply a cold pack or ice in a dry plastic bag. NOTE: Application of heat has two purposes: 1) it may mask the perception of pain; and 2) it may assist in thermolysis. Since we know the venom is a protein that has been superficially inoculated, application of heat may help by denaturing the toxin.
Always seek an emergency medical evaluation.
Continue monitoring the patient until a higher level of care has been reached.
Vinegar Application
Use of vinegar is controversial with Physalia spp. Though the use of vinegar has traditionally been recommended, several studies both in-vivo and in-vitro show massive nematocyst discharge upon pouring household vinegar over certain species of cnidarians, including Physalia. Still, the most current American Heart Association guidelines (AHA 2010) recommend application of vinegar for all jellyfish, including Physalia spp. If anything changes, DAN will let you know.
If you do choose to apply vinegar, you can optimize application and significantly economize by using spray bottles. Generously spray the area with vinegar for no less than 30 seconds to neutralize any invisible remnants. Pick off any remaining tentacles.
Lionfish
The lionfish is a genus of venomous fish commonly found in tropical reefs. Native to the Indo-Pacific, the fish is one of the most infamous invasive species in the western Atlantic. This voracious predator is not a threat to divers, but its introduction into exotic ecosystems can decimate juvenile specimens. In an attempt to control the spread of lionfish populations, recreational divers in the Americas have started aggressive campaigns to hunt them; in the process, many divers are stung with the lionfish’s sharp spines, which can cause very painful and sometimes complicated wounds.
Identification and Distribution
Lionfish, turkeyfish and zebrafish are common names for fish species of the genus Pterois, a subset of fish of the venomous Scorpaenidae family. Though lionfish are native to the Indo-Pacific, members of the family Scorpaenidae can be found in oceans all over the globe, even in arctic waters. Lionfish specimens are typically red with white and black stripes and have showy, spiky fins. Species include Pterois volitans, P. miles, P. radiata, and P. antenata among a few others.
Western Atlantic Invasion
Since the early 1990s, invasive lionfish have wreaked havoc on local juvenile reef fish populations in the western Atlantic. Out of the nine species of Pterois, only P. volitans and P. miles are found in Western Atlantic waters, but they range from as far north as Rhode Island down to Venezuela and The Guianas.
Risk to Humans
Knowing no predators, these fish are generally docile, allowing divers to approach closely enough and making themselves easy targets for spearfishing. Unfortunately, the desperate attempts to eradicate these fish from the Americas have caused a significant rise in the incidence of lionfish puncture wounds.
Epidemiology
The prevalence and incidence of lionfish envenomations is unknown. Treating physicians may not choose to consult a poison control center, and in the United States are under no obligation to report these injuries to state or federal agencies. Scientific literature accounts for 108 cases of lionfish envenomations reported between 1976 and 2001, and almost all of these reports are actually from marine aquarists. It is impossible to know how often victims go untreated and how often treatment goes unreported, but the frequency of case reports seems to indicate that lionfish envenomations are not uncommon.
Lionfish culling tournaments are becoming more and more popular all over the Caribbean. Recent studies conducted by DAN staff from Cozumel, Mexico accounted over four years of tournaments. Incidence of injury during these events was between 7-10% of participants.
Mechanism of Injury
Most lionfish-related incidents occur as a result of careless handling, usually during spearfishing or while preparing them for consumption. Lionfish have needlelike spines located along the dorsal, pelvic and anal fins, and punctures can be extremely painful and lead to rapid development of localized edema and subcutaneous bleeding. Pain can last for several hours, edema typically resolves in two to three days, and tissue discoloration can last up to four or five days. Due to edema and the venom’s inherent toxicity, puncture wounds on fingers can lead to ischemia (restriction of blood supply to the tissues) and necrosis.
Prevention
Lionfish are by no means aggressive. To prevent injuries, maintain a prudent distance. If you are committed to engage in spearfishing or culling activities, avoid improvisations and do not try to handle these animals until you learn from more experienced divers.
First Aid
If you are stung, remain calm. Notify the dive leader and your buddy. The priority is to safely end your dive, returning to the surface following a normal ascent rate. Do not skip any decompression obligation.
On the surface, first aid providers should:
Rinse the wound with clean freshwater.
Remove any obvious foreign material.
Control bleeding if needed. It is ok to allow small punctures to bleed for a minute immediately after being stung (this may decrease venom load).
Apply heat. Immerse the affected area in hot water (upper limit of 113°F/45°C) for 30 to 90 minutes. If you are assisting a sting victim, try the water on yourself first to assess tolerable heat levels. Do not rely on the victim’s assessment, as intense pain may impair his ability to evaluate tolerable heat levels. If you cannot measure water temperature, a good rule of thumb is to use the hottest water you can tolerate without scalding. Note that different body areas have different tolerance to heat, so test the water on the same area where the diver was injured. Repeat if necessary. NOTE: Thermolysis can also be a secondary benefit worth pursuing, but it tends to be less effective in cases where the venom has been injected deep into the tissues.
Apply bandaging as needed.
Seek a professional medical evaluation.
Blue-Ringed Octopus
Blue-ringed octopus are a small species of venomous octopi that live in tropical tide pools from south Japan to the coastal reefs of Australia and the western Indo-Pacific. These small octopi are the only cephalopods known to be dangerous to humans.
Identification
The blue-ringed octopus hardly ever exceeds eight inches (20 centimeters) in size. Their most distinctive feature is the blue iridescent rings that cover their yellow-colored body; however, it is important to emphasize that this feature is only displayed when the animal is disturbed, hunting or mating. When calm or at rest, the animal may display an overall yellowish, grey or beige coloration without any visible blue rings. The blue-ringed octopus is more active at night, spending most of the day hidden in its nest in shallow areas or tide pools.
Epidemiology
Blue-ringed octopus envenomations are very rare. These animals are only endemic to southern Japan, Australia and the western Indo-Pacific. Cases outside of this region are generally due to deliberate handling of aquarium specimens. There are only a handful of reported fatal cases. Full recovery is expected with timely professional medical intervention.
Mechanism of Injury
As with all cephalopods, octopi have a strong beak similar to those of parrots and parakeets. All octopi have some sort of venom to paralyze their victims, but the blue-ringed octopus bite may contain an extremely powerful neurotoxin called tetrodotoxin (TTX), which can be up to 10,000 times more potent than cyanide and can paralyze a victim in minutes. Theoretically, a little over one-half milligram of this venom—the amount that can be placed on the head of a pin—is enough to kill an adult human. Certain bacteria present in the blue-ringed octopus’ salivary glands synthesize the toxin. TTX is not unique to the blue-ringed octopus; certain newts, dart frogs, cone snails and pufferfish can also be a source of TTX intoxication, though from different mechanisms.
Signs and Symptoms
A blue-ringed octopus bite is usually painless or no more painful than a bee sting; however, even painless bites should be taken seriously. Neurological symptoms dominate every stage of envenomation, and manifest as paresthesia (tingling and numbness) progressing to paralysis that could potentially culminate in death. If envenomation has occurred, signs and symptoms usually start within minutes and may include paresthesia of the lips and tongue. This is usually followed by excessive salivation, trouble with pronunciation (dysarthria), difficulty swallowing (dysphagia), sweating, dizziness and headache. Serious cases may progress to muscular weakness, incoordination, tremors and paralysis. Paralysis may eventually affect respiratory muscles, which can lead to severe hypoxia with cyanosis (blue or purple tissue discoloration due to insufficient oxygen in the blood).
Prevention
These animals are not aggressive, and divers should not fear blue-ringed octopi. If encountered, avoid handling these animals. Due to their small size and lack of skeleton, a blue-ringed octopus den might be a small space only accessible through a tiny crevice, so avoid picking up bottles, cans or mollusk shells in areas they inhabit.
First Aid
Care is supportive. There is no antivenom available. If someone is bitten:
Clean the wound with freshwater and provide care for a small puncture wound.
Apply the pressure immobilization technique. NOTE: TTX is a heat-stable toxin, so the application of heat will not denature the toxin.
Watch for signs and symptoms of progressive paralysis.
Be prepared to provide mechanical ventilations with a bag valve mask device or a manually triggered ventilator.
Do not wait for signs and symptoms of paralysis. Always seek an evaluation at the nearest emergency department. NOTE: The bite site might be painless and still be lethally toxic.
Wound excision is never recommended.
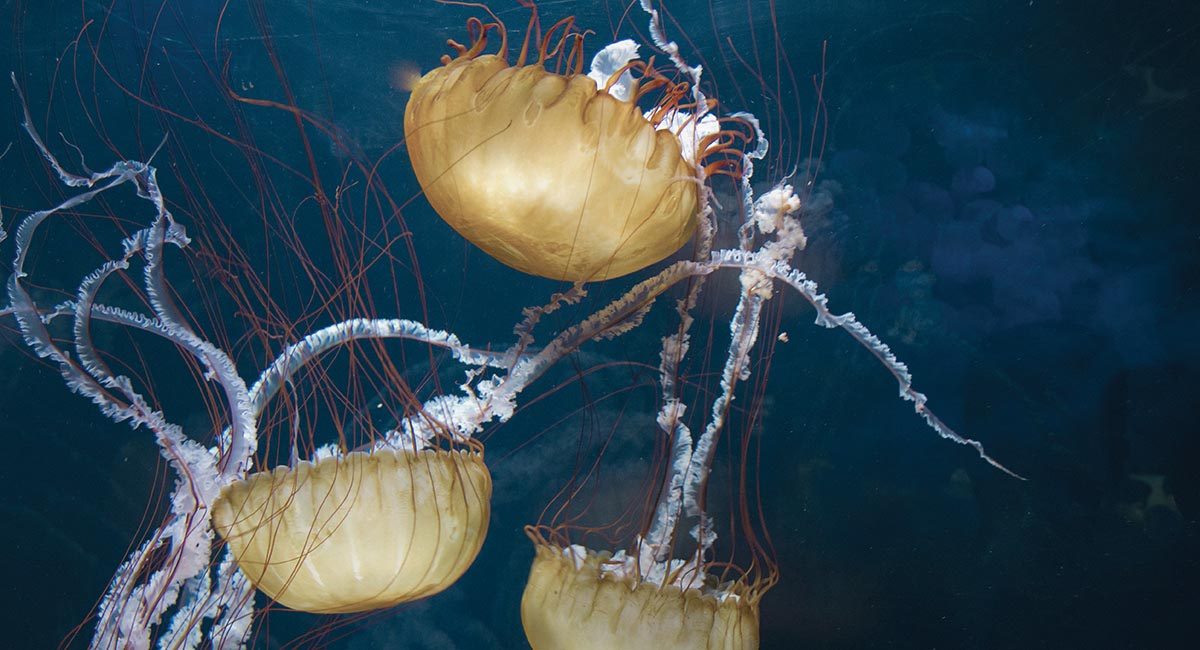
Box Jellyfish
Box jellyfish (cubozoans) are cube-shaped medusa notorious for possessing one of the most potent venoms known to mankind. Certain species can kill an adult human in as little as three minutes, scarcely enough time for any rescue response.
Biology and Identification
Medusas are the migrant form of cnidarians. In the case of box jellyfish, their bell-like body is cube shaped, with tentacles extending from each corner. Box jellyfish are complex animals with a propulsion mechanism and a relatively sophisticated nervous system for a jellyfish. They have up to 24 eyes, some of them with corneas and retinas, enabling them to not only detect light but also to see and circumnavigate objects to avoid collision.
While some jellyfish live off of symbiotic algae, box jellyfish prey on small fish, which are immediately paralyzed upon contact with their tentacles. Then the tentacles are retracted, carrying the prey into the bell for digestion. Some species hunt daily, and at night some species can be observed resting on the ocean floor.
Epidemiology and Distribution
From 1884 to 1996, there were more than 60 reported fatalities from box jellyfish stings in Australia. There are species of box jellyfish in almost all tropical and subtropical seas, but life-threatening species seem to be restricted to the Indo-Pacific.
Notorious Species
SEA WASP
Found in the coastal waters of Australia and Southeast Asia, sea wasp is the common name for the most dangerous cnidarian: Chironex fleckerii. The largest cubozoan, sea wasps have a bell approximately eight inches (20 centimeters) in diameter and tentacles ranging from a few centimeters to up to 10 feet (three meters). Contact with these animals triggers the most powerful and lethal envenomation process known to science. Sea wasp envenomation causes immediate excruciating pain followed by cardiac failure. Death may occur in as little as three minutes.
Recent studies have identified a component of the venom that drills a hole in red blood cells, causing a massive release of potassium, possibly responsible for the lethal cardiovascular depression. The same study may have also identified a way to inhibit this effect, which in the coming years could prove to be clinically promising.
FOUR-HANDED BOX JELLYFISH
The four-handed box jellyfish (Chiropsalmus quadrumanus) habitat spans from South Carolina to the Caribbean, the Gulf of Mexico and as far south as Brazil. The four-handed box jellyfish can inflict extremely painful stings and is the slightly smaller American cousin to the Australian sea wasp. There is one documented case of a four-year-old boy who was stung in the Gulf of Mexico and died within 40 minutes.
BONAIRE BANDED BOX JELLYFISH
Bonaire banded box jellyfish (Tamoya ohboya) is a relatively unknown, highly venomous species found in the Dutch Caribbean. Since 1989, there have been roughly 50 confirmed sightings primarily in Bonaire with the remainder on the shores of Mexico, St. Lucia, Honduras, St. Vincent and the Grenadines. There have only been three reported cases of envenomation, which lead to intense pain and skin damage; only one case required hospitalization.
IRUKANDJI SYNDROME
Tiny box jellyfish found near Australia, Carukia barnesi and Malo kingi, are responsible for the infamous and extremely painful symptomatic complex known as Irukandji syndrome. These small cubozoans’ bells are only a few millimeters with tentacles up three feet (one meter). Fortunately, fatalities from these smaller species are rare, but stings are extremely painful and can cause systemic symptoms including cardiovascular instability that should prompt immediate medical attention. Survivors have reported a feeling of impending doom, claiming they were certain that they could not survive such intense, generalized pain; however, it is important to emphasize that a single sting should not be fatal.
Though stings from lesser-known species of cubozoans are not necessarily lethal, they can still be very painful. An immediate medical evaluation is always recommended.
Prevention
Properly research the areas you intend to dive.
Avoid known box jellyfish habitats if you are not sure the dive site or swimming area is safe. If stung, cardiovascular stability can rapidly deteriorate with very little time for any effective field intervention.
In Northern Queensland, Australia, net enclosures are placed in the water where box jellyfish are known to be during summer months (November to May), but these cannot guarantee safety.
Minimize unprotected areas. Always wear full wetsuits, hoods, boots and gloves. Something as simple as nylon pantyhose worn over the skin will prevent jellyfish stings.
Carry sufficient household vinegar with you to all dive sites.
First Aid
If stung by any jellyfish, follow these procedures in this order:
Activate local emergency medical services.
Monitor victim’s airway, breathing and circulation. Be prepared to perform CPR at any moment (particularly if you suspect box jellyfish).
Avoid rubbing the area. Box jellyfish tentacles can be cylindrical or flattened, but they are coated with cnydocites, so rubbing the area or allowing the tentacles to roll over the skin will exponentially increase the affected surface area and the envenomation process.
Apply household vinegar to the area. Generously pour or spray the area with vinegar for no less than 30 seconds to neutralize any invisible remnants. You can pour the vinegar over the area or use a spray bottle, which optimizes application. Let the vinegar stand for a few minutes before doing anything else. NOTE: This will not do anything to the pain or the venom already injected, but it is intended to stabilize any remaining unfired nematocysts on the diver’s skin before you try to remove them.
Wash the area with seawater (or saline). Use a syringe with a steady stream of water to help remove any tentacle remains. Do not rub. NOTE: Do not use freshwater; this could cause massive nematocyst discharge.
Apply heat. Immerse the affected area in hot water (upper limit of 113°F/45°C) for 30 to 90 minutes. If you are assisting a sting victim, try the water on yourself first to assess tolerable heat levels. Do not rely on the victim’s assessment, as intense pain may impair his ability to evaluate tolerable heat levels. If you cannot measure water temperature, a good rule of thumb is to use the hottest water you can tolerate without scalding. Note that different body areas have different tolerance to heat, so test the water on the same area where the diver was injured. Repeat if necessary. If hot water is not available, apply a cold pack or ice in a dry plastic bag. NOTE: Application of heat has two purposes: 1) it may mask the perception of pain; and 2) it may assist in thermolysis. Since we know the venom is a protein that has been superficially inoculated, application of heat may help by denaturing the toxin.
Always seek an emergency medical evaluation.
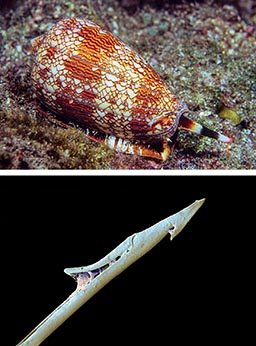
Cone Snails
Cone snails are marine gastropods characterized by a conical shell and beautiful color patterns. Cone snails possess a harpoon-like tooth capable of injecting a potent neurotoxin that can be dangerous to humans.
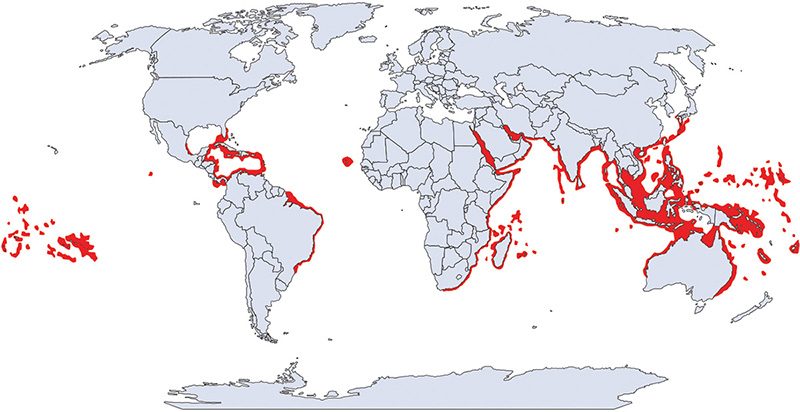
Identification and Distribution
There are about 600 different species of cone snails, all of which are poisonous. Cone snails live in shallow reefs partially buried under sandy sediments, rocks or corals in tropical and subtropical waters. Some species have adapted to colder waters.
Mechanism of Injury
Injuries typically occur when the animal is handled. Cone snails administer stings by extending a long flexible tube called a proboscis and then firing a venomous, harpoonlike tooth (radula).
Signs and Symptoms
A cone snail sting can cause mild to moderate pain, and the area may develop other signs of acute inflammatory reaction like redness and swelling. Conustoxins affect the nervous system and are capable of causing paralysis possibly leading to respiratory failure and death.
Epidemiology
The prevalence and incidence of cone snails envenomations is unknown, but it is probably a very rare occurrence in divers and the general population. Shell collectors (professional or amateur) may be at higher risk.
Prevention
If you see a beautiful marine snail that looks like a cone, it is probably a cone snail. It is difficult to tell whether a cone snail inhabits a given shell as they are able to hide inside them. Since all cone snails are venomous, err on the side of safety and do not touch it.
First Aid
Unfortunately, there is no specific treatment for cone snail envenomations. First aid focuses on controlling pain, but may not influence outcomes. Envenomation will not necessarily be fatal, but depending on the species, the amount of venom injected, and the victim’s size and susceptibility, complete paralysis may occur and this may lead to death. Cone snail venom is a mixture of many different substances including tetrodotoxin (TTX).
Clean the wound with freshwater and provide care for a small puncture wound.
Apply the pressure immobilization technique. NOTE: Application of heat might help with pain management, but since TTX is a heat-stable toxin, the application of heat will not denature the toxin.
Watch for signs and symptoms of progressive paralysis.
Be prepared to provide mechanical ventilations with a bag valve mask device or a manually triggered ventilator.
Do not wait for signs and symptoms of paralysis. Always seek an evaluation at the nearest emergency department. NOTE: The bite site might be painless and still be lethally toxic.
“Wash thoroughly, use soap and keep it clean and dry.”
Bites account for the majority of marine life associated trauma. Fortunately, serious encounters are extremely rare. Traumatic injuries are usually the result of an animal’s defensive reaction to a perceived threat or misidentification of a diver’s body part as a food source. Most puncture wounds do not contain venom and are, therefore, a traumatic injury. Bleeding is the most common acute complication to trauma, while infections are the most common secondary complication. In this chapter, we will cover the more common traumatic injuries, how to prevent them and how to properly manage them.
An abrasion is a superficial scrape that occurs when the skin is rubbed or bumped against a rough object.
Epidemiology
Skin abrasions, minor skin cuts and scrapes are very common among recreational divers. Accidental contact with rocks, corals, wrecks and other hard surfaces in or around dive sites can cause injury. Divers with poor buoyancy control frequently report abrasions. In addition, divers who dive close to the bottom or through narrow passageways without the protection of full-length wetsuits often report minor abrasions on their lower extremities.
Risks to Divers
Skin abrasions expose your underlying tissues to microorganisms, significantly increasing the risk of infections. Bleeding can also be of concern, particularly when the injury occurs on highly perfused areas like your face, head, hands and fingers.
Prevention
To avoid skin abrasions, you must master buoyancy control and use mechanical protection like gloves and full-body wetsuits. Though thermal insulation may not be necessary in tropical dive destinations, protection from potential skin abrasions as well as from stinging microscopic life is always a good idea. It is important to note that in an attempt to protect underwater fauna, gloves might not be permitted at some dive destinations. Ask the local dive operator about its protocols before wearing gloves; it may help to explain your reasons for wanting to wear them.
First Aid
In case of minor skin abrasions, follow these basic first aid guidelines:
Wash the area thoroughly with clean freshwater (sterile if available).
Apply antiseptic solution (iodine-based antiseptic solutions may be contraindicated in patients with hyperthyroidism).
Control bleeding by applying direct pressure with a sterile bandage.
If bleeding has been controlled:
Let the area dry out.
Apply triple antibiotic ointment.
Cover the area with a sterile bandage.
Have the wound evaluated by a medical professional within 24 hours to assess risk of infections.
If bleeding persists:
Cover the wound with clean dressings and keep them in place.
Continue to apply pressure.
Seek an immediate medical evaluation.
Treatment
For abrasions or amputations with significant bleeding, contact local emergency medical services immediately, apply bleeding control techniques and monitor the patient’s vital signs. Be prepared to manage shock.
Stingrays
Stingrays are shy, peaceful fish. They do not represent a threat to divers unless startled, stepped on or deliberately corralled and threatened. Most injuries occur in shallow waters when divers or swimmers are walking in areas where stingrays reside.
Biology and Identification
Rays are closely related to sharks: class Chondrichthyes, chondr- meaning cartilaginous and -ichthyes meaning fish. It’s important to note that not all rays have stingers. Stingrays are a specific group of rays classified in the suborder Myliobatoidei, which consists of eight families: deep water stingrays, sixgill stingrays, stingarees, round rays, butterfly rays, river stingrays, eagle rays and whiptail stingrays.
The approximate stingray wingspan varies across species from one foot to more than six feet (two meters). Some freshwater species can weigh up to 1,300 pounds (600 kilograms).
Distribution
There are species of stingrays in nearly all oceans. Some families consist of only freshwater species, which are typically found in tropical, subtropical and temperate river environments.
Mechanism of Injury
Stingrays are not aggressive by any means, and injuries are rarely fatal. The stingray’s defense mechanism consists of a serrated barb at the end of its tail with venom glands located at the base of the barb. The venom is a variable mixture of substances, none of which are specific to the animal; therefore, the creation of antivenom is not possible. Stingrays will strike when threatened or stepped on. The barb can easily tear wetsuits and penetrate skin, and may cause deep, painful lacerations.
Epidemiology
It is estimated that stingrays are responsible for approximately 1,500 accidents each year in the United States. Prevalence on other countries might be higher, particularly injuries associated with freshwater species, but epidemiological data is either elusive or inexistent.
Signs and Symptoms
Stingrays can inflict mild to severe puncture wounds or lacerations. The initial symptom is pain, which can be significant and intensify over several hours. Both puncture wounds and lacerations can damage major blood vessels causing severe, potentially life-threatening bleeding. The barb usually breaks off and may require professional surgical care.
It is common for stingray wounds to become infected despite proper care. Notable possible infections include cellulitis, myositis, fasciitis and tetanus.
Prevention
Avoid stepping in murky or low-visibility shallow waters where stingrays naturally inhabit.
Stingrays often burrow in the sand, making them difficult to see even in tropical waters.
If you are shore diving and you suspect there may be stingrays, carefully shuffle your feet while entering or exiting the water. This technique is known as the “stingray shuffle.” Stingrays are very sensitive animals, and the vibrations caused by this shuffling may scare them away.
First Aid
Clean the wound thoroughly.
Control bleeding if necessary.
Do not delay professional medical evaluation. The risk for tetanus and other serious infections must be professionally minimized.
Sea Urchins
Sea urchins are typically small, rounded spiny creatures found on shallow rocky marine coastlines. The primary hazard associated with sea urchins is contact with their spines.
Biology and Identification
Sea urchins are echinoderms, a phylum of marine animals shared with starfish, sand dollars and sea cucumbers. Echinoderms are recognizable, because their pentaradial symmetry (they have five rays of symmetry), which is easily observed on a starfish. This symmetry corresponds with a water vascular system used for locomotion, transportation of nutrients and waste, and respiration. Sea urchins have tubular feet called pedicellariae, which enable movement. In one genus of sea urchin— the Flower Sea Urchin—some of the pedicellariae have evolved into toxic claws. In this species, the spines are short and harmless, but these toxic claws can inflict an envenomation.
Sea urchins feed on organic matter in the seabed. Their mouth is located on the base of their shell and their anus is on the top. The color of sea urchins varies depending on the species—shades of black, red, brown, green, yellow and pink are common.
Distribution
There are species of sea urchins in all oceans from tropical to arctic waters. Most human-sea urchin incidents occur in tropical and subtropical waters.
Mechanism of Injury
Sea urchins are covered in spines, which can easily penetrate divers’ boots and wetsuits, puncture the skin and break off. These spines are made of calcium carbonate, the same substance that comprises eggshells. Sea urchin spines are usually hollow and can be fragile, particularly when it comes to extracting broken spines from the skin. Injuries usually happen when people step on them on while walking across shallow rocky bottoms or tide pools. Divers and snorkelers are often injured while swimming on the surface in shallow waters as well as when entering or exiting the water from shore dives.
Epidemiology
Although little epidemiological data is available, sea urchin puncture wounds are common among divers, particularly when in shallow waters, near rocky shores or in close proximity to wrecks and other hard surfaces. The DAN Medical Information team receives at least one call a week regarding sea urchin injuries, typically from divers and snorkelers swimming in very shallow waters near rocky shores.
Signs and Symptoms
Sea urchin
Injuries are typically in the form of puncture wounds, often multiple and localized. Skin scrapes and lacerations are also possible. Puncture wounds are generally painful and associated with redness and swelling. Pain ranges from mild to severe depending on several factors, including the species, the body area of the wound, joint or muscular layers compromised, number of punctures, depth of puncture, and the individual’s threshold for pain. Multiple puncture wounds may cause limb weakness or paralysis, particularly with the long-spined species of the genus Diadema. On very rare occasions, immediate life-threatening complications may occur.
Prevention
Be observant while entering or exiting the water from shore dives, particularly when the bottom is rocky.
If swimming, snorkeling or diving in shallow waters, near rocky shores or in close proximity to wrecks and other hard surfaces, maintain a prudent distance and buoyancy control.
Avoid handling these animals.
First Aid
There is no universally accepted treatment for sea urchin puncture wounds. Both first aid and definitive care is symptomatic.
Apply heat. Immerse the affected area in hot water (upper limit of 113°F/45°C) for 30 to 90 minutes. If you are assisting a sting victim, try the water on yourself first to assess tolerable heat levels. Do not rely on the victim’s assessment, as pain may impair his ability to evaluate tolerable heat levels. If you cannot measure water temperature, a good rule of thumb is to use the hottest water you can tolerate without scalding. Note that different body areas have different tolerance to heat, so test the water on the same area where the diver was injured. Repeat if necessary. NOTE: Very few species of sea urchins contain venom. If present, hot water immersion may also help denature any superficial toxins.
Remove any superficial spines. Tweezers can be used for this purpose; however, sea urchin spines are hollow and can be very fragile when grabbed from the sides. Your bare fingers are a softer alternative to hard tweezers. NOTE: Do not attempt to remove spines embedded deeper in the skin; let those be handled by medical professionals. Deeply embedded spines may break down into smaller pieces, complicating the removal process.
Wash the area thoroughly, but avoid forceful rubbing and scrubbing if you suspect there may still be spines embedded in the skin.
Apply antiseptic solutions or over-the-counter antibiotic ointments if available.
Do not close the wound with tape or glue; this might increase the risk of infection. NOTE: Deep puncture wounds are the perfect environment to culture an infection, particularly tetanus.
Regardless of any first aid provided, always seek a professional medical evaluation.
Treatment
Contrary to popular belief, very few species of sea urchins are actually toxic. Pain and swelling is often the result of the body’s reaction to myriad different antigens present on the surface of the spines.
Spines are usually covered with strong pigments, so individual puncture wounds are often clearly visible and may cause suspicion that each puncture contains a fragment of a spine. Though this is possible, it may not necessarily be the case. It is easier to assess each individual puncture once the acute inflammatory process has started to recess.
The decision of whether or not surgical removal of retained spines is necessary is usually based on joint or muscular layer involvement, and whether there is pain with movement or signs of infection. Spines will usually encapsulate in a short time, but they may not always dissolve. A reactive granuloma is a common reaction to remaining small foreign bodies. Radiological localization, fluoroscopy or an ultrasound might be useful to avoid a blind surgical extraction that may cause further spine fracture.
The use of anti-inflammatories and physical therapy is often key for managing these injuries, particularly when they involve small joints as a prolonged inflammatory process may result in fibrosis, which may limit range of motion. If signs of infection are present, the doctor may prescribe antibiotics and a tetanus booster.
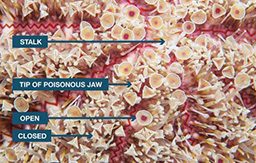
Flower Sea Urchin
The Flower Sea Urchin (Toxopneustes spp.) is the most toxic of all sea urchins. Its short spines are harmless, but its pedicellariae, which look like small flowers, are tiny claws (Toxopnueustes, meaning toxic foot). These claws contain a toxin that can cause severe pain similar to that of a jellyfish sting, faint giddiness, difficulty breathing, slurred speech, generalized weakness, and numbness of the lips, tongue and eyelids.