Q: When I go on a dive vacation, we often have beers or cocktails after diving. Some in the group are even suggesting drinks between dives — is that a bad idea?
A: Simply put, alcohol and diving are not compatible. Alcohol causes depression of the central nervous system, which impairs judgment and reduces reaction time and coordination. Often the individual is not even aware of the degree of impairment.
A review of more than 15 studies on the effects of alcohol on performance found that alcohol was involved in roughly 50 percent of all accidents in people of drinking age. In Diving and Subaquatic Medicine (Edmonds C, et al., 2002), the authors report that alcohol is associated with up to 80 percent of all drownings in adult males.
It takes time for alcohol to be metabolized and its effects to wear off. M.W. Perrine and colleagues studied a group of experienced divers and the impact of alcohol consumption on their performance. Their investigation found that the ability to perform skills while scuba diving was significantly compromised at a blood alcohol concentration (BAC) of 0.04 percent, which can be reached by a 180-pound man who consumes two 12-ounce beers in one hour on an empty stomach. The study went on to state that even at a lower BAC, situational awareness and protective inhibitions may be reduced.
Recent alcohol intake (along with seasickness, traveler’s diarrhea, excessive sweating, diuretic medications and air travel) is a potential cause of dehydration in divers. Dehydration, particularly when severe, is a potential risk factor for decompression sickness (DCS). Diving can also contribute to further fluid loss through breathing dry air and diuresis caused by both immersion and cold. Some symptoms of dehydration, such as fatigue or drowsiness, can even mimic DCS, leading to possible diagnostic confusion.
Alcohol ingestion may also enhance the effects of nitrogen narcosis. Elevated BAC, dehydration and nitrogen narcosis together may result in otherwise preventable accidents due to decreased problem-solving ability.
Many divers appreciate a cold beer, but drinking and diving can turn a safe activity into a nightmare for both the diver and all those impacted by a rescue or fatality. Think twice before combining alcohol and diving.
Q: I have been getting advice from lots of people about what kind of drops to put in my ears after diving. What does DAN have to say?
A: Ear drops are not necessary postdive for most divers.
The purpose of most ear drops is to prevent external ear-canal infections (known as otitis externa or swimmer’s ear). Infections of the ear canal are associated with persistent moisture as well as local skin trauma, which can result from insertion of cotton swabs or other objects into the ears. (These can damage the thin skin that lines the ear canal. As DAN medics are fond of saying, “Don’t put anything smaller than your elbow in your ear.”) These factors can enable bacterial overgrowth and infection.

Difficulty equalizing, clicking or crackling sounds and feelings of fullness or fluid in the ears probably indicate a mild or moderate barotrauma of the middle ear. Middle-ear barotrauma is neither treated nor helped by drops placed in the ear canal, as the injury exists on the other side of the eardrum. An intact eardrum forms a barrier that will prevent the drops from reaching the middle ear. A perforated eardrum might allow drops to enter the middle ear, but this would not help and could be harmful.
For divers plagued by swimmer’s ear, gently rinsing the ears with fresh water after each dive may help. Drying the ears with a hair dryer (taking care the air is not too hot) may also be helpful. If these methods are not effective, the next step is using commercially available eardrops to limit persistent moisture. Common ingredients in these formulations can include acetic acid (the active ingredient in vinegar), boric acid, aluminum acetate, sodium acetate, isopropyl alcohol and glycerin. The acids alter pH, which retards bacterial growth; aluminum acetate and sodium acetate are astringents, which shrink tissues. Isopropyl alcohol helps dry the tissues, and glycerin may help lubricate the skin and prevent excessive drying.
Any diver who experiences ear symptoms after diving — especially pain, hearing loss or tinnitus (ringing/buzzing sound) — should discontinue diving and be evaluated by a doctor. Prompt treatment may prevent further irritation or infection and may expedite a return to the water. Learn more about your ears and how to take care of them with DAN’s online seminar “Ears and Diving,” available at www.DAN.org.
Q: Last fall I underwent a pulmonary vein ablation for atrial fibrillation. Five months later my cardiologist ordered an echocardiogram with bubble study to confirm closure of the puncture in my interatrial septum. Unfortunately, the hole persists. The cardiologist admitted to an incomplete understanding of the relevant issues but recommended I refrain from diving until closure of the hole can be confirmed or it is surgically repaired. What can you tell me about my fitness to dive?
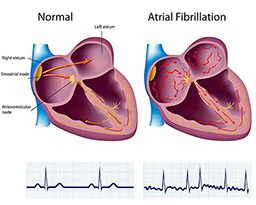
A: Atrial fibrillation (a-fib) is one of the most common rhythm disorders encountered in clinical cardiology. Basically, the atria (upper chambers of the heart) quiver rather than contracting in an organized fashion. This leads to a very rapid and irregular heart rhythm that can be quite uncomfortable (though some people do not experience symptoms) and may put patients at a significantly increased risk for stroke. Risk factors for the development of a-fib are hypertension, underlying coronary artery disease, increasing age and valvular heart disease.
In the past, the intention of therapy was to either slow the rate of the fibrillation (using drugs or catheter-based radiofrequency ablation) or control the rhythm with drugs. Success rates at maintaining normal rhythm over the next year were generally less than 50 to 70 percent.
Atrial fibrillation can now be treated in selected patients with catheter-based isolation of the pulmonary veins in the left atrium. This procedure has a long-term success rate of about 80 percent, but it requires the cardiologist to puncture the interatrial septum to get from the right atrium to the left atrium. The hole or holes usually close spontaneously over time, but they don’t always. Until they are closed the patient is left with an atrial septal defect of sorts — similar to a congenital “hole in the heart.” This means venous bubbles might bypass the lungs (which act as bubble filters) and cross into arterial circulation. This would put a diver at an increased risk of decompression illness (DCI). Information is limited, but the increase in risk seems to be about fivefold and is likely related to the size of the hole or holes. Although that may sound like a dramatic increase, the risk of DCI in recreational diving is about 2 per 10,000 dives. Thus, a fivefold increase in this risk is only 1 per 1,000 dives — still a very low absolute risk.
The primary concern with respect to one’s risk of DCI isn’t the hole, it’s the bubble load. Thus, the cautious thing to do is to minimize your bubble load by diving conservatively. If you were my patient, I would support recreational diving on the richest nitrox mix allowable for your depth with prolonged safety stops using the same mix or a richer mix if your level of certification allows. I definitely would NOT recommend closing the hole before returning to diving; the risk of significant complication from that procedure is around 1 percent, which is much higher than the risk of DCI with leaving it alone (0.1 percent).
While it is reasonable to wait and see if it closes spontaneously before you return to diving, it is also reasonable to resume diving (with the caveats listed) despite the defect, knowing there is an increased, albeit small, absolute risk of DCI.
— Douglas Ebersole, M.D.
Q: I do a lot of diving; as a result of handling tanks, lines, ladders and other gear, I usually have a cut or two somewhere — typically on my hands. Should I be concerned about getting an infection while diving?

A: Skin is the body’s primary barrier against infection. Breaks in the skin, therefore, enable skin bacteria and the abundance of microscopic life in seawater to contaminate vulnerable subdermal (beneath the skin) tissues.
The diving environment can compromise skin integrity. Prolonged immersion and high humidity may alter the skin’s pH and soften the outer layer of the epidermis, causing peeling (desquamation), further reducing the skin’s natural defenses and enabling infection — overgrowth of bacteria or other microorganism within a wound. For cuts and scrapes that occur in or around water (including lakes, streams and oceans) thorough cleaning with soap and water is recommended, followed by the application of a protective dressing. People with open wounds should refrain from entering the water until healing is complete. Maintain an up-to-date tetanus vaccination to minimize risk of infection by that pathogen.
© Alert Diver — Q3 Summer 2012