In case of an emergency during a dive trip, who should I call first: DAN® or local emergency services? I was surprised when the DAN representative I spoke to immediately after a recent incident told me to call 911 first and then call back. I thought DAN would coordinate any needed rescue.

DAN’s evacuation coverage is often misunderstood. Worldwide, DAN always works with and through local agencies. In general, a member who is injured, whether from a diving, swimming, snorkeling or land-based incident, should always attempt to involve local resources first. For incidents on land or near shore, this typically means calling emergency medical services (EMS), the police or fire department, park services or other relevant resources. For a diving incident, a dive boat must generally access land to get an injured diver the help he or she needs. People can call DAN at any time in an emergency, but the first call should be to 911 (or the designated EMS number for the country in which the incident occurs), the coast guard, the marine emergency channel or similar.
According to the DAN member handbook:
Emergency Evacuation does not include efforts to locate an injured person whose location is unknown or efforts to rescue such persons from a dangerous situation or a location inaccessible by emergency services personnel. Emergency Evacuation may begin only after the injured person is made available at a location that can be reached by emergency medical services personnel.
— Frances Smith, EMT-P, DMT
I could not find any information on your website about the use of a menstrual cup while diving. Is it safe? Is there any research or recommendation about it?
Diving with a menstrual cup is considered safe. The air spaces of concern while diving are those that have the potential to trap gas — the lungs, ears, sinuses, gastrointestinal tract and those that sometimes occur around dental work. Overexpansion occurs when an air space takes on gas at depth and that air expands during ascent to greater than the original volume. Thus, air spaces that have no exposure to compressed gas are not a concern. Any air in a menstrual cup will be compressed as you descend and then expand to its original size upon ascent.
Women who use menstrual cups generally have no problems with physical activities such as diving. Manufacturers of these devices report that occasional problems arise with new users who do not get the cup seated correctly, which results in leakage. They suggest it may take several cycles for women to master the insertion process and determine the proper cup size. If you are well versed and comfortable in the use of a menstrual cup, no issues should arise during a dive.
A common suggestion is to empty the cup prior to activity. If you plan to dive from a boat, check out the boat’s available facilities in advance. Toilets, privacy and hand-washing options may be limited. Boat dives often involve a half day or more at sea, so advanced planning should help alleviate unnecessary hassle or embarrassment.
The larger concern would be any ancillary problems associated with menstruation — headache, abdominal cramping, irritability, etc. While these symptoms may not be debilitating, they can still compromise dive safety. In a 2006 study of 420 women by Marguerite St Leger Dowse and colleagues, 81 percent reported premenstrual tension, and 40 percent felt that their ability to perform was impaired. These researchers also found that feelings of panic, anxiety, loss of control, dizziness and cold were more pronounced in divers who were menstruating.
For women who are feeling well and are not suffering from ancillary symptoms, diving with a menstrual cup should not present any additional dive safety concerns.
— Lana Sorrell, EMT, DMT, and Frances Smith, EMT-P, DMT

I have varicose veins, which I want to have removed. Will this procedure present any problems relative to diving?
Removing varicose veins does not present any particular problems for divers. No specific procedure is recommended for divers, because there is no need for any special consideration. Your doctor should use the procedure that best suits your clinical needs. A return to diving is appropriate after you have fully recovered from the procedure and you are released for full and unrestricted activity.
— Marty McCafferty, EMT-P, DMT
I have hearing loss and tinnitus in both ears; the condition is most likely hereditary. I want to try scuba diving, but with these ear issues I am not sure I should. Can I dive? Should I see a specialist first?
Whether someone with hearing loss and/or other hearing problems should dive is debated among professionals with relevant expertise. Some experts suggest that a person with preexisting hearing problems should not dive. This opinion is based on the idea that all divers place their hearing at risk of various injuries. Most of these injuries are preventable, but risk still exists. People with hearing loss are not necessarily at greater risk of injury than others, but the outcome of an injury might have much greater repercussions (e.g., total deafness).

Other experts believe that if a potential diver fully understands and accepts the risks, he or she can consider diving. The risk involved is not quantifiable. Call the DAN medical information line at +1 (919) 684-2948 to learn more about the various ways ears can be injured in the dive environment. Speak with a knowledgeable local dive instructor who can help you make an objective risk-versus-benefit analysis and tell you the injury-mitigation strategies you would learn in dive training. Finally, raise your concerns with your doctor or an ear, nose and throat (ENT) specialist. Please feel free to encourage the doctor to call DAN to discuss your situation.
— Marty McCafferty, EMT-P, DMT
I had a spontaneous pneumothorax when I was 18. I am now 48. Is the contraindication for scuba diving permanent? I was the classic case — a tall, skinny teenager at the tail end of a rapid growth spurt. I had a chest tube for two or three days, but I have had no related issues in 30 years.
Please note that DAN is not a regulatory agency and does not set physical standards or guidelines for scuba diving. The responsibility for the decision about whether to dive is generally left up to the individual and his or her physician. This decision, however, should be an informed decision based on a medical evaluation and a solid understanding of all the risks involved.
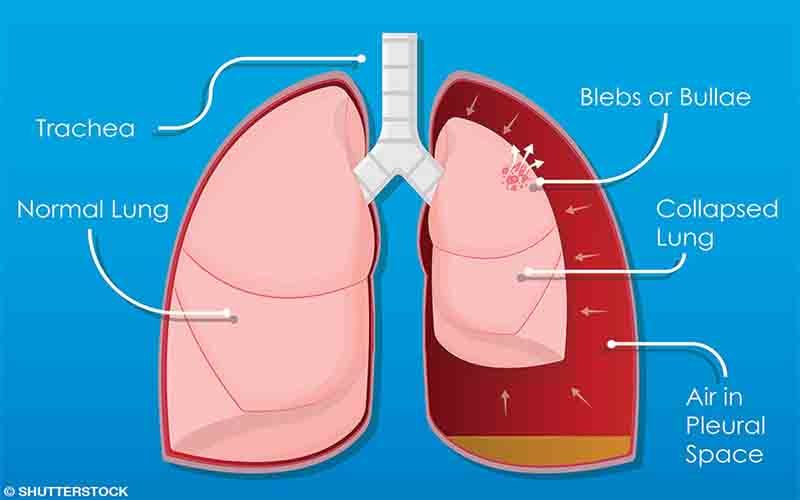
A history of a spontaneous pneumothorax is generally considered an absolute contraindication to diving. Some individuals have inherent weak areas in the pleural lining of their lungs that may take the form of small blisters or outpouchings of the lungs; these are called blebs. The spots are weaker than the normal lining of the lung and can occasionally break and cause air to leak from the lung into the chest cavity. When this happens, the result is a spontaneous pneumothorax: unexpected rupture of alveoli (lung air sacs).
Such a lung collapse can occur without provocation and with no warning. Often the individual is exercising, straining while lifting or performing some other physical task, but sometimes the person is doing nothing out of the ordinary.
Since barotrauma can occur with hyperinflation of lung tissue, a diver’s lungs must be able to tolerate rapid changes in volume and pressure. Fibrotic or scarred tissue is of particular concern to the scuba diver because it offers reduced compliance in its interface with normal lung tissue. Any weakness in lung structure or architecture may be predisposed to rupture from even minimal overinflation. Pulmonary barotrauma usually happens near the end of a dive.
Escaped gas from the lungs can enter one of three places:
- The mediastinal area around the heart (causing pneumomediastinum or mediastinal emphysema)
- The pleural space between the lung and the chest wall (causing pneumothorax)
- The bloodstream (causing arterial gas embolism)
Presence of blebs and smoking seem to be risk factors for spontaneous pneumothorax. A person who has had a spontaneous pneumothorax has a 30 percent chance of having another within two to three years. There is a further 30 percent chance of recurrence after three years, with a 60 percent long-term risk for another pneumothorax. These statistics are based on the finding that a person who has pleural blebs usually has more than one, and all blebs are prone to leaking at some point.
Diving, unlike above-water activities, involves pressures likely to stimulate a bleb to rupture and leak air into the chest cavity. A spontaneous pneumothorax that occurs underwater is much more likely to be fatal than one that occurs above water. Because of the increased risk of such an event during a dive and the possibility of a severe pneumothorax if gas expands in the chest during ascent, the expert consensus is that people who have ever had a spontaneous pneumothorax should not dive.
— Frances Smith, EMT-P, DMT