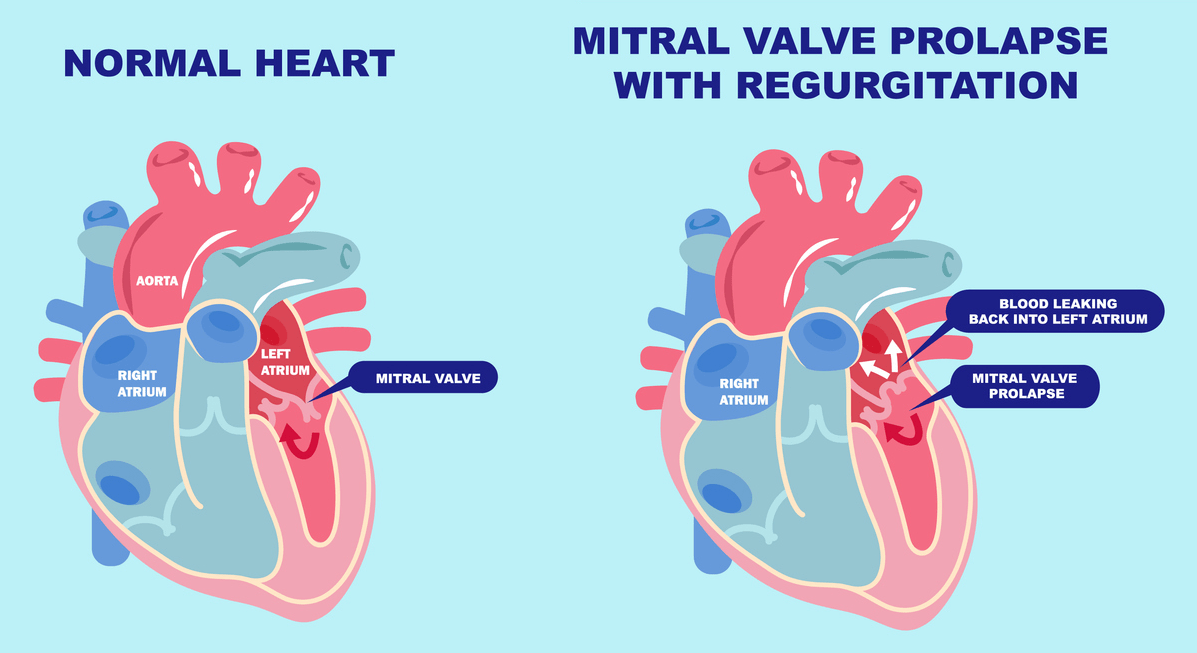
Mitral valve prolapse (MVP) is a condition in which the mitral valve — which allows blood to flow from the left atrium into the left ventricle — does not close properly, resulting in a backflow of blood called regurgitation. This can cause a characteristic murmur during auscultation. MVP is also known as “floppy valve syndrome” or “click-blow syndrome” and is more common in women.
The mitral valve has two leaflets. MVP is characterized by the expansion and contraction of one or both of these leaflets towards the left atria. If severe, then blood may pass or reflux and cause mitral reguritation. The causes of MVP are uncertain, but there are two forms: primary (usually hereditary) and secondary (associated with other diseases). Primary MVP may result from thick valves, irregular surfaces, or issues with tendon fibers. Secondary MVP is linked to additional diseases affecting blood flow, heart muscle function, or valve structure.
Doctors alternatively classify MVP as “flaccid valve syndrome” or “click-murmur syndrome.” This condition is common, particularly among women. MVP presents with a wide wide range of symptoms, which can include chest discomfort, an unexpected sensation in the chest during each beating, minimal or no symptoms, or even a myocardial infarction. Transitory loss of consciousness or a mild stroke (called “transitory ischemic attacks”) is another risk factor associated with MVP.
Understanding MVP
Understanding the potential risks for individuals with MVP who wish to scuba dive requires understanding the condition itself. MVP occurs when the mitral valve, which regulates blood flow between the left heart’s chambers, does not close properly. This faulty closure allows blood to leak backward into the left atrium, leading to symptoms like chest pain, fatigue, and heart palpitations. While MVP is typically benign, certain factors can increase the risk of complications: severe valve regurgitation, a family history of MVP-related complications, and an enlarged left atrium. Individuals with MVP should undergo regular cardiology check-ups to monitor their heart health and function.
Risks Associated with Diving with MVP
People with MVP should consider potential risks before scuba diving. The sport involves descending to depths where pressure increases significantly, placing additional strain on the heart and potentially causing complications. Individuals with MVP are at a higher risk of experiencing arrhythmias, abnormal heart rhythms, and the physical exertion involved in scuba diving can further increase the risk of arrhythmias.
Precautions for Individuals with MVP
If you have MVP and are considering diving, take certain precautions to minimize potential risks. Here are some key guidelines:
- Consult with your healthcare provider: Prior to engaging in scuba diving, it is crucial to have a thorough discussion with your healthcare provider. They can assess your overall cardiac health and provide specific recommendations based on your individual case.
- Obtain clearance from a cardiologist: It is advisable to seek clearance from a cardiologist who specializes in dive medicine. They can perform a comprehensive evaluation of your heart function, including an echocardiogram, to determine if scuba diving is safe for you.
- Limit depth and dive duration: To reduce the risk of barotrauma and strain on the heart, individuals with MVP should limit their dives to shallow depths and shorter durations. Adhering to recreational dive limits is essential for your safety. Avoid engaging in strenuous or high-intensity diving activities such as deep dives, wreck dives, or cave exploration, which can place excessive strain on the heart.
- Monitor symptoms closely: Pay close attention to any symptoms such as chest pain, shortness of breath, palpitations, or dizziness during or after diving. If you experience any of these symptoms, it is important to seek medical attention immediately.
By following these precautions, individuals with MVP can enjoy a safe and fulfilling scuba diving experience. Always prioritize your health and safety and consult with medical professionals who can guide you through the process.
Consulting with Healthcare Professionals
One of the most crucial aspects of ensuring safety when diving with MVP is consulting with healthcare professionals. The expertise and guidance they provide can significantly reduce the risks associated with the condition.
First and foremost, it is essential to have an open and honest discussion with your primary healthcare provider. They can assess your overall cardiac health and provide specific recommendations based on your individual case. Additionally, they may refer you to a cardiologist who specializes in dive medicine. Obtaining clearance from a cardiologist is highly advisable before diving. These experts can perform a comprehensive evaluation of your heart function, including an echocardiogram, to determine if it is safe for you to dive.
Everyone’s case is unique, and healthcare professionals may provide varying advice. It is important to follow their guidance closely and communicate any concerns or symptoms you may experience during or after diving. By prioritizing communication with healthcare professionals, you can enjoy a safe and enjoyable scuba diving experience.
Safety Measures: Diving with MVP
While consulting with healthcare professionals is crucial before diving with MVP, there are also important safety measures to consider. These measures can further minimize the risks associated with MVP and help ensure a safe and enjoyable dive.
- Monitor your body’s response before, during, and after each dive. Pay close attention to any symptoms, such as palpitations, shortness of breath, chest discomfort, or dizziness. If you experience any of these symptoms, ascend to a shallower depth or end the dive.
- Stay properly hydrated. Dehydration can exacerbate MVP symptoms and increase the risk of underwater complications. Drink enough fluids before your dive to start with optimal hydration levels. Replenish fluids afterward, as immersion causes diuresis.
- Do not over-hydrate before your dive, as this can also cause complications.
- Dive within your limits and avoid excessive exertion. Pace yourself, conserve your energy, and avoid engaging in strenuous activities that may put unnecessary stress on your heart. Listen to your body’s signals.
By following these safety measures, including consulting with your healthcare professional, and remaining vigilant during your diving adventures, you can enjoy the wonders of the underwater world while managing the risks associated with MVP. Always prioritize your safety and exercise caution.
Implications in Diving
For the Diver
- Individuals diagnosed with MVP may need to take certain precautions to address potential cardiovascular effects.
- Consult with a healthcare provider, preferably one with expertise in diving medicine, before engaging in scuba diving with a MVP diagnosis.
- Undergo a thorough cardiovascular evaluation, including stress testing, to assess your fitness for diving.
- Monitor symptoms, such as palpitations or chest pain, and promptly address any new or worsening symptoms.
- Be cautious about specific medications and their potential interactions with diving-related conditions, and discuss them with a healthcare provider.
- Ensure adequate hydration and avoid excessive caffeine intake when engaged in diving.
- Cardiovascular health and fitness to dive can be a dynamic state. Regular follow-ups with a healthcare provider are essential to assessing the ongoing management of MVP and making any necessary adjustments to the diving plan.
For the Dive Operator
- As expedition leader, you have the duty to take care of your clients if they present any discomfort during the dive trip.
- If customer discloses any cardiovascular condition, make sure your customers are medically fit to dive.
- Consider the risks involved in remote dive operations and live-aboards; where timely access to advanced diagnostic procedures and interventions cannot be guaranteed.
- Don’t worry about getting a hold of a doctor with dive medicine experience; although a cardiologist would be ideal, any doctor should be able to help as a first step. If this primary care physician deems necessary, they will refer this patient to a specialist.
- Do offer the examining physician to contact DAN for consultation.
- tions for dive operators include:
For the Physician
- MVP is a condition in which the mitral valve leaflets protrude into the left atrium during ventricular systole due to their laxity. This can lead to mitral regurgitation and puts individuals at higher risk of infective endocarditis, atrial fibrillation, arrhythmias, stroke, and sudden cardiac death (Delling, F. N. 2014). MVP is relatively common, affecting 2–3% of the general population (Freed et al., 1999). It often presents without symptoms and is discovered incidentally during physical examination when a mid-systolic click and late systolic murmur are auscultated.
- It has been estimated that recreational dives (Buzzacott, P. 2014) without complications require moderate energy — generally a 7-MET capacity (peak VO2 24.5 mL/kg/min in men and 22.4 mL/kg/min in women) is sufficient (Buzzacott, P. 2014). However, it is advisable for divers to maintain higher aerobic fitness levels to ensure adequate energy reserves.
- The risks of scuba diving depend greatly on the severity of MVP and associated medical conditions. After evaluation, individuals with uncomplicated MVP and no associated conditions often receive clearance for recreational scuba diving, while those with moderate or severe MVP may face restrictions due to heightened risks. Some governing bodies, such as the South Pacific Underwater Medicine Society (SPUMS), have put forth guidelines regarding fitness to dive with MVP. They recommend that asymptomatic individuals with click/murmur MVP without arrhythmias, an enlarged left atrium, or significant mitral regurgitation can dive cautiously with extra surveillance. However, those with moderate or severe prolapse, symptoms, or a history of endocarditis or arrhythmias may be restricted from diving even recreationally.
- The primary concerns with MVP and diving involve arrhythmias triggered by exertion underwater and rapid pressure changes affecting an already compromised mitral valve. Uncomplicated MVP presents a low risk of issues during recreational diving. However, as MVP severity increases, so does the risk of complications underwater; thus, a close evaluation by a dive medicine specialist is warranted. All divers with MVP should undergo thorough annual exams to assess new-onset arrhythmias, the progression of valvular dysfunction, and clearance for continued diving activity.
- Individuals diagnosed with MVP should undergo annual cardiology monitoring to identify any high risk features mentioned or to track the development of mitral regurgitation.
- In summary, mild MVP is usually compatible with recreational scuba diving from a cardiac standpoint. However, moderate or severe MVP warrantscaution and evaluation by a dive medicine specialist to assess fitness to dive. All divers with MVP should have regular follow-up to monitor for progression of valve dysfunction or new arrhythmias that could pose underwater risks. With proper surveillance and evaluation, many people with this common valve condition can safely continue recreational scuba diving.
References
- Freed, L.A., Levy, D., Levine, R.A., Larson, M.G., Evans, J.C., Fuller, D.L., & Benjamin, E.J. (1999). Prevalence and clinical outcome of mitral-valve prolapse. New England Journal of Medicine, 341(1), 1–7.
- Delling, F. N., & Vasan, R. S. (2014). Epidemiology and Pathophysiology of Mitral Valve Prolapse: New Insights Into Disease Progression, Genetics, and Molecular Basis. Circulation, 129(21), 2158-2170. doi:10.1161/circulationaha.113.006702
- Buzzacott, P., Pollock, N. W., & Rosenberg, M. (2014). Exercise intensity inferred from air consumption during recreational scuba diving. Diving and hyperbaric medicine, 44(2), 74–78.