It is not uncommon for divers to complain of pain or tenderness in the jaw, a headache or aching facial pain after diving. The gripping action required to hold a mouthpiece in place may strain the muscles used for chewing (masticatory muscles) or the temporomandibular joint (TMJ), which connects the jaw (mandible) to the temporal bone. Pain associated with the TMJ and masticatory muscles is known as temporomandibular dysfunction (TMD).
“During diving, the TMJ is subjected to a stress equal to what you would experience if you kept your mouth open — not fully, but as if you stuck three fingers into it vertically — during the entire dive,” said Costantino Balestra, Ph.D., vice president of research and education at DAN Europe. “This acts on the retromeniscal neurovascular bundle and can cause myalgia or headache. By having a customized mouthpiece molded, this can be reduced or even eliminated.” Balestra is the lead author of the study “Scuba diving can induce stress of the temporomandibular joint leading to headache,” published in the British Journal of Sports Medicine in 2004.
The most common mouthpiece designs feature an elliptical airway attached to the demand valve, a labial flange to provide stability and a platform the diver bites for retention. Mouthpieces generally feature short bite tabs and are made of a soft material to accommodate use by a wide range of jaws and teeth; this requires forward movement of the jaw to effectively grip the mouthpiece. This design may not support posterior occlusion, which is the most effective contact of the molar and bicuspid teeth of both jaws for allowing the natural movements of the jaws essential to normal chewing and closure. This lack of support may result in uneven loading of the TMJ. Cold water may exacerbate this problem by impairing a diver’s ability to use his or her lips to properly grip the mouthpiece.
Understanding TMD
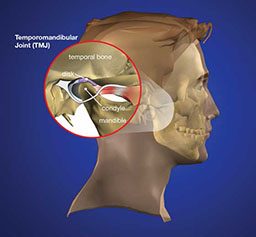
The TMJ is one of the most complex joints in the body; its movement involves a combination of hinging and sliding action. To locate it, place a finger directly in front of your ears. Move your jaw from side to side, or open and close your mouth. You can actually feel the mandible moving in and out of the TMJ socket. The upper section of the joint is a depression in the temporal bone of the skull; the lower section of the joint is the mandibular condyle, a rounded projection at the upper tip of the mandible. These bones, which make up the joint, are covered in cartilage and are separated by a small disc, which facilitates smooth opening, closing and side-to-side movements.

In many cases, the cause of TMD is not clear. TMD may occur if this disc erodes or becomes improperly aligned, if the cartilage is damaged by arthritis or if the joint is subjected to trauma or long-term microtraumas. Researchers are still seeking to fully understand the causes of these conditions and what treatments are most effective.
Reported symptoms include:
- pain or tenderness in the TMJ
- TMJ clicking or crepitus (cracking or popping sound)
- discomfort while chewing
- difficulty opening or closing the mouth
- facial pain
- headache
- blockage of Eustachian tubes
- vestibular disturbances such as vertigo or disorientation (either of which could be hazardous should it occur underwater)
Several studies have noted more women reporting TMD symptoms than men. The average age of onset is between 20 and 40, but this dysfunction may occur at any age. In their study “Prevalence of temporomandibular dysfunction in a group of scuba divers,” Aldridge and Fenlon suggest that this may be related to anatomical differences such as mandibular angulation and masticatory muscle insertion.
Scuba diving does not appear to cause TMD; however, it may exacerbate a preexisting joint condition. “The problem is that there are many people who have silent or undiagnosed conditions or just plain flimsy joints, which only become symptomatic when the stress of holding a traditional mouthpiece is imposed,” said Dr. Randall Moles, orthodontic specialist and developer of the SeaCureTM custom mouthpiece (one of several commercially available custom mouthpieces). “So there is a group of people who will have no TMD symptoms prior to diving who can develop TMJ problems because they had weak joints or a preexisting subclinical problem.”
What You Can Do
There are a few styles of standard mouthpieces designed for scuba diving. When selecting your diving equipment, try several mouthpieces to find the style and size that fits you best. For added comfort, some divers add a second-stage swivel adaptor to their regulator that adjusts to subtle head movements and reduces hose tug. Some regulators incorporate this adaptor as standard design.

If you experience symptoms of TMD during or after diving, seek a dental consultation. While most cases of diving-associated TMD resolve spontaneously, your dental professional can recommend management strategies such as muscle relaxation exercises, techniques for reducing stress or, if necessary, medical intervention. Your dentist can also advise or assist in the development of a custom-fitted mouthpiece, which requires less muscular effort for retention than the traditional design. (There are also commercially available custom mouthpieces that do not require a dental consultation).
“The dive industry has tried to make a mouthpiece that will fit everyone, and in doing so they had to make it soft and short due to the variability of teeth and jaws,” Moles said. “A customized mouthpiece is molded to fit one person and can be made out of a stiffer material that goes to the back of the mouth, which transfers the weight of the regulator to the back — where the muscles are. This provides leverage and greatly reduces the force needed to keep the mouthpiece in place. In addition, because the mouthpiece can be made of a much stiffer material, it retains the bite marks that grip the teeth instead of the diver having to constantly bite down to get a grip on the soft spongy material of the standard mouthpiece.”
If you opt for a custom-fitted mouthpiece, consider the proper positioning for a diver. “There is a common mistake made during the molding: People keep their head in the neutral position,” Balestra noted. “This will not mold the mouthpiece correctly; instead the individual should position his head as if he was diving, tilting the head backward.”
Safety Considerations
If you decide to swap your mouthpiece for a custom one, make sure your new mouthpiece fits your regulator’s second stage. Not every mouthpiece fits every regulator, and an ill-fitting mouthpiece could incur leakage or decouple from the regulator. In addition, when attaching your mouthpiece with a cable tie, confirm tightness, and use a razor blade to cut off excess and ensure there are no sharp ends.
Do not use a customized mouthpiece on an air source that might be handed off to a buddy in an emergency; it may make breathing difficult or be impossible for another diver to use.
© Alert Diver — Q1 Winter 2014