Oxygen administration is an important early first aid measure for divers with suspected decompression illness (DCI). The goal is to deliver oxygen at the highest possible oxygen concentration while being mindful of oxygen supply limits. Oxygen systems commonly used for dive accidents can have two delivery options: a pressure-activated demand valve or constant flow for use with a nonrebreather mask.
The demand valve has been promoted as an easy-to-use system that conserves the oxygen supply since it releases oxygen only when the user inhales. Recent research, however, found that the nonrebreather mask set at 15 liters per minute can provide better tissue oxygenation than the demand valve with an oronasal mask.1 Researchers suspected that poor mask fit led to the underperformance of the demand valve. This article will summarize an evaluation of different mask configurations to determine if they influence the oxygen delivery fraction when breathing with the demand valve.2
Methods

Sixteen healthy volunteer divers (both male and female) tested four different mask configurations: an adult soft silicone oronasal mask (Tru-Fit mask by Allied Health Care Products Inc.), a pocket face mask with air cushion (Sturdy Industrial Co.), and an intraoral mask (NuMask) with a nose clip and without a nose clip.
The dead space volume, representing the volume of gas that will be breathed (or rebreathed) from a sealed mask, was measured prior to testing. Oxygenation was measured in three different ways: the fraction delivered to the mouth (inspired oxygen fraction (FiO2), the fraction reaching the back of the throat (nasopharynx) and tissue oxygen levels measured through skin transcutaneous oximetry. Sensors were taped on six standard sites on the arms and legs, the skin was warmed to ensure good blood flow, and the levels of tissue oxygen were recorded at regular intervals throughout the oxygen breathing periods. After the oxygen breathing, the participants rated each mask configuration on comfort, ease of breathing and ease of holding the device in place.
Results
The oxygen fraction delivered to the mouth was similar for all configurations. The nasopharyngeal FiO2 was significantly higher with the intraoral mask (both with and without the nose clip) than with the pocket face mask or silicone oronasal mask. The tissue oxygen levels achieved were statistically similar for the intraoral mask both with and without the nose clip. The silicone oronasal mask delivered statistically lower tissue oxygen levels (Figure 1).
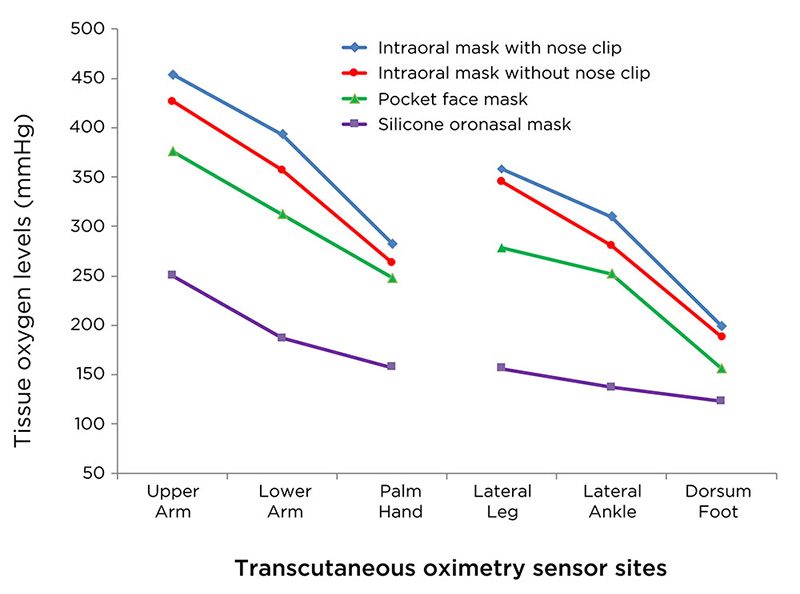
Participants rated the pocket face mask as the most comfortable and the nose clip as very uncomfortable. They described the intraoral mask (like a scuba regulator mouthpiece) as the easiest to use since it rests in the mouth when the subjects are lying on their backs. Constant pressure was required to maintain a seal with the other two masks. The intraoral mask had a very small dead space volume (14 milliliters), meaning little gas would be rebreathed. The dead space was eight times larger for the pocket face mask and 14 times larger for the silicone oronasal mask.
Discussion
The demand oxygen delivery system was designed to provide effective first aid oxygen to injured divers. Evaluating tissue oxygen levels is the best way to assess oxygen delivery effectiveness. Our findings confirm that the type of mask used with the oxygen delivery system can affect performance. Both the intraoral mask and the pocket face mask were superior to the silicone oronasal mask in performance. The intraoral mask with a nose clip offered the best performance but not statistically better than the intraoral mask without a nose clip.
Divers are accustomed to breathing through a mouthpiece, so the intraoral mask is easy to use, and facial hair and face shape do not interfere with the fit. It is easy to hold in place and continued to maintain a good seal under a wide range of conditions.
The large dead space volume of the oronasal mask has both positive and negative effects. While the large volume can serve as a reservoir for the oxygen supply, it also means that there is more rebreathing of expired gas, diluting the fresh oxygen supply with expired carbon dioxide. Fidgeting with the mask can introduce more surrounding air that can dilute the inspired oxygen fraction. There is much less expired gas rebreathing or ambient air dilution with the intraoral mask.
The intraoral and pocket face masks come with a filter and one-way valve that allows the masks to be used for mouth-to-mouth resuscitation in a nonbreathing diver. The filter and one-way valve assembly need to be removed before attaching these masks to the demand valve.
Conclusion
We tested three commonly available oxygen masks used with a demand valve for first aid oxygen delivery. Of these, the intraoral mask with a nose clip obtained the highest tissue and inspired oxygen levels in healthy divers when used with a demand valve. Oxygen values were similar for the intraoral mask with and without the nose clip. Given the reported discomfort of the nose clip, the use of the intraoral mask without the nose clip may be the best of the options tested.
References
- Blake DF, Naidoo P, Brown LH, Young D, Lippmann J. A comparison of the tissue oxygenation achieved using different oxygen delivery devices and flow rates. Diving Hyperb. Med. 2015; 45(2):79-83.
- Blake DF, Crowe M, Lindsay D, Brouff A, Mitchell SJ, Pollock NW. Comparison of tissue oxygenation achieved breathing oxygen from a demand valve with four different mask configurations. Diving Hyperb. Med. 2018; 48(4):209-17.
About the Authors:
Denise F. Blake, M.D., is an emergency and dive physician in Townsville, Queensland, Australia. This research is part of her current doctoral program at James Cook University. Neal W. Pollock, Ph.D., is an associate professor of kinesiology at Université Laval in Québec, Canada.
© Alert Diver — Q4 2019