While exciting, observing marine life in their environment comes with a risk. Injuries, though rare, may occur as a result of an uninformed swimmer or diver’s actions. The Hazardous Marine Life reference book examines the most common hazardous marine life that water enthusiasts may encounter and introduces the mechanisms of injury, techniques for injury prevention and application of first aid.
Envenomation is a process by which a venom or toxin is injected into another being via a bite, puncture or sting. Envenomation is always due to direct contact with an animal (or parts of it like drifting jellyfish tentacles). There are two possible mechanisms of injection: active, such as jellyfish or cone snails, or passive like lionfish or sea urchins. Injuries typically occur during shore entries or exits, incidental contact or deliberate attempts to handle a specimen. Envenomations are rare but can be life-threatening and may require rapid first aid response. In this chapter, we will cover some common envenomations as well as some of the more rare, but serious cases.
Fire corals are colonial marine cnidarians that when touched can cause burning skin reactions. Fire coral-related incidents are common among divers with poor buoyancy control.
Biology and Identification
Fire coral, which belong to the genus Millepora, are found in tropical and subtropical waters around the world. Generally fire coral adopts a yellow-green or brownish branchy formation, although its external appearance often varies due to environmental factors. Because fire coral can colonize hard structures, it can even adopt a rather stony appearance with rusty coloration.
Despite their calcareous structure, fire coral is not a true coral; these animals are more closely related to Portuguese man-of-war and other hydrozoans.
Mechanism of Injury
Fire coral gets its name because of the fiery sensation experienced after coming into contact with a member of the species. The mild to moderate burning that it causes is the result of cnydocites embedded in its calcareous skeleton; these cnydocites contain nematocysts that will fire when touched, injecting their venom.
Signs and Symptoms
The burning sensation may last several hours and is often associated with a skin rash that appears minutes to hours after contact. This skin rash can take several days to resolve. Often, the skin reaction will subside in a day or two, but it may likely reappear several days or weeks after the initial rash disappeared.
Fire coral lacerations, in which an open wound receives internal envenomation, are the most problematic fire coral injuries. Venom from Millepora spp. is known to cause tissue necrosis on the edges of a wound. These injuries should be carefully observed, as necrotic tissue provides a perfect environment to culture serious soft tissue infections.
Fire coral are found in tropical and subtropical waters around the world.
Prevention
Avoid touching these calcareous formations.
If you need to kneel on the bottom, look for clear sandy areas.
Remember that hard surfaces such as rocks and old conchs may be colonized by fire coral even if they do not look branchy.
Always wear full-body wetsuits to provide protection against the effects of contact.
Master buoyancy control.
Always look down while descending.
First Aid
Rinse the affected area with household vinegar.
Redness and vesicles will likely develop. Do not puncture them; just let them dry out naturally.
Keep the area clean, dry and aerated—time will do the rest.
For open wounds, seek a medical evaluation. NOTE: Fire coral venom is known to have dermonecrotic effects. Share this information with your physician before any attempts to suture the wound, as the wound edges might become necrotic.
Antibiotics and a tetanus booster may be necessary
Portuguese Man-of-War
Portuguese man-of-wars are free-floating cnidarians characterized by blue gas-filled bladders and long tentacles that drift on the surface of the ocean. Contact with a man-of-war’s tentacles can cause intense pain and other systemic symptoms.
Biology and Identification
There are two species for the genus: Physalia physalis in the Atlantic and Physalia utriculus in the Indo-Pacific. The Atlantic man-of-war may reach slightly larger dimensions, with the gas bladder rarely exceeding one foot (30 centimeters) and tentacles averaging 33 feet (10 meters) and possibly extending up to 165 feet (50 meters).
Though many people mistake the Portuguese man-of-war for species of jellyfish, this genus belongs to the order Siphonophora, a class of hydrozoans. What we see as a single specimen is actually a colony composed of up to four different types of polyps. Despite its resemblance, these animals are more closely related to fire coral than to jellyfish.
The Portuguese man-of-war is easily recognizable; if you see blue tentacles, you can bet they belong to Physalia.
Risk to Humans
The man-of-war’s polyps contain cnidocytes delivering a potent proteic neurotoxin capable of paralyzing small fish. For humans, most stings cause red welts accompanied by swelling and moderate to severe pain. These local symptoms last for two to three days.
Systemic symptoms are less frequent, but potentially severe. They may include generalized malaise, vomiting, fever, elevated heart rate at rest (tachycardia), shortness of breath and muscular cramps in the abdomen and back. Severe allergic reactions to the man-of-war’s venom may interfere with cardiac and respiratory function, so divers should always seek a timely professional medical evaluation.
Epidemiology
Approximately 10,000 cnidaria envenomations occur each summer off the coasts of Australia, the vast majority of which involve Physalia. In fact, man-of-wars cause the most cnidarian envenomations prompting emergency evaluation globally. The risk may not be so great for divers, however, as most Physalia stings occur on beaches or on the surface of the water rather than while submerged. Certain regions are known to have seasonal outbreaks, but incidence is highly variable between regions.
Prevention
Always look up and around while surfacing. Pay special attention during the last 15-20 feet of your ascent, since this is the area where you may find cnidarians and their submerged tentacles.
Wear full body wetsuits regardless of water temperature. Mechanical protection is the best way to prevent stings and rashes.
In areas where these animals are known to be endemic, a hooded vest may be the best way to protect your neck.
First Aid
Avoid rubbing the area. Cnidarian tentacles are like nematocyst-coated spaghetti, so rubbing the area or allowing the tentacles to roll over the skin will exponentially increase the affected surface area and, therefore, the envenomation process. NOTE: Initial pain may be intense. Though life-threatening complications are rare, monitor circulation, airway and breathing, and be prepared to perform CPR if necessary.
Remove the tentacles. You must take great care to remove the man-of-war’s tentacles in order to avoid further envenomation. Those distinctive blue tentacles are quite resistant to traction, so you can remove them fairly easily with some tweezers or gloves. NOTE: If you do not have access to tweezers or gloves, the skin on your fingers is likely thick enough to protect you. Keep in mind, however, that after removal your fingers may contain hundreds or even thousands of unfired nematocysts, so pretend you have been handling hot chili peppers that cause blisters anywhere you touch and treat your fingers as recommended from the next step on.
Flush the area with seawater. Once the tentacles and any remnants have been removed, use a high volume syringe and flush the area with a powerful stream of seawater to remove any remaining unfired nematocysts. Never use freshwater since this will cause unfired nematocysts to fire.
Apply heat. Immerse the affected area in hot water (upper limit of 113°F/45°C) for 30 to 90 minutes. If you are assisting a sting victim, try the water on yourself first to assess tolerable heat levels. Do not rely on the victim’s assessment, as intense pain may impair his ability to evaluate tolerable heat levels. If you cannot measure water temperature, a good rule of thumb is to use the hottest water you can tolerate without scalding. Note that different body areas have different tolerance to heat, so test the water on the same area where the diver was injured. Repeat if necessary. If hot water is not available, apply a cold pack or ice in a dry plastic bag. NOTE: Application of heat has two purposes: 1) it may mask the perception of pain; and 2) it may assist in thermolysis. Since we know the venom is a protein that has been superficially inoculated, application of heat may help by denaturing the toxin.
Always seek an emergency medical evaluation.
Continue monitoring the patient until a higher level of care has been reached.
Vinegar Application
Use of vinegar is controversial with Physalia spp. Though the use of vinegar has traditionally been recommended, several studies both in-vivo and in-vitro show massive nematocyst discharge upon pouring household vinegar over certain species of cnidarians, including Physalia. Still, the most current American Heart Association guidelines (AHA 2010) recommend application of vinegar for all jellyfish, including Physalia spp. If anything changes, DAN will let you know.
If you do choose to apply vinegar, you can optimize application and significantly economize by using spray bottles. Generously spray the area with vinegar for no less than 30 seconds to neutralize any invisible remnants. Pick off any remaining tentacles.
Lionfish
The lionfish is a genus of venomous fish commonly found in tropical reefs. Native to the Indo-Pacific, the fish is one of the most infamous invasive species in the western Atlantic. This voracious predator is not a threat to divers, but its introduction into exotic ecosystems can decimate juvenile specimens. In an attempt to control the spread of lionfish populations, recreational divers in the Americas have started aggressive campaigns to hunt them; in the process, many divers are stung with the lionfish’s sharp spines, which can cause very painful and sometimes complicated wounds.
Identification and Distribution
Lionfish, turkeyfish and zebrafish are common names for fish species of the genus Pterois, a subset of fish of the venomous Scorpaenidae family. Though lionfish are native to the Indo-Pacific, members of the family Scorpaenidae can be found in oceans all over the globe, even in arctic waters. Lionfish specimens are typically red with white and black stripes and have showy, spiky fins. Species include Pterois volitans, P. miles, P. radiata, and P. antenata among a few others.
Western Atlantic Invasion
Since the early 1990s, invasive lionfish have wreaked havoc on local juvenile reef fish populations in the western Atlantic. Out of the nine species of Pterois, only P. volitans and P. miles are found in Western Atlantic waters, but they range from as far north as Rhode Island down to Venezuela and The Guianas.
Risk to Humans
Knowing no predators, these fish are generally docile, allowing divers to approach closely enough and making themselves easy targets for spearfishing. Unfortunately, the desperate attempts to eradicate these fish from the Americas have caused a significant rise in the incidence of lionfish puncture wounds.
Epidemiology
The prevalence and incidence of lionfish envenomations is unknown. Treating physicians may not choose to consult a poison control center, and in the United States are under no obligation to report these injuries to state or federal agencies. Scientific literature accounts for 108 cases of lionfish envenomations reported between 1976 and 2001, and almost all of these reports are actually from marine aquarists. It is impossible to know how often victims go untreated and how often treatment goes unreported, but the frequency of case reports seems to indicate that lionfish envenomations are not uncommon.
Lionfish culling tournaments are becoming more and more popular all over the Caribbean. Recent studies conducted by DAN staff from Cozumel, Mexico accounted over four years of tournaments. Incidence of injury during these events was between 7-10% of participants.
Mechanism of Injury
Most lionfish-related incidents occur as a result of careless handling, usually during spearfishing or while preparing them for consumption. Lionfish have needlelike spines located along the dorsal, pelvic and anal fins, and punctures can be extremely painful and lead to rapid development of localized edema and subcutaneous bleeding. Pain can last for several hours, edema typically resolves in two to three days, and tissue discoloration can last up to four or five days. Due to edema and the venom’s inherent toxicity, puncture wounds on fingers can lead to ischemia (restriction of blood supply to the tissues) and necrosis.
Prevention
Lionfish are by no means aggressive. To prevent injuries, maintain a prudent distance. If you are committed to engage in spearfishing or culling activities, avoid improvisations and do not try to handle these animals until you learn from more experienced divers.
First Aid
If you are stung, remain calm. Notify the dive leader and your buddy. The priority is to safely end your dive, returning to the surface following a normal ascent rate. Do not skip any decompression obligation.
On the surface, first aid providers should:
Rinse the wound with clean freshwater.
Remove any obvious foreign material.
Control bleeding if needed. It is ok to allow small punctures to bleed for a minute immediately after being stung (this may decrease venom load).
Apply heat. Immerse the affected area in hot water (upper limit of 113°F/45°C) for 30 to 90 minutes. If you are assisting a sting victim, try the water on yourself first to assess tolerable heat levels. Do not rely on the victim’s assessment, as intense pain may impair his ability to evaluate tolerable heat levels. If you cannot measure water temperature, a good rule of thumb is to use the hottest water you can tolerate without scalding. Note that different body areas have different tolerance to heat, so test the water on the same area where the diver was injured. Repeat if necessary. NOTE: Thermolysis can also be a secondary benefit worth pursuing, but it tends to be less effective in cases where the venom has been injected deep into the tissues.
Apply bandaging as needed.
Seek a professional medical evaluation.
Blue-Ringed Octopus
Blue-ringed octopus are a small species of venomous octopi that live in tropical tide pools from south Japan to the coastal reefs of Australia and the western Indo-Pacific. These small octopi are the only cephalopods known to be dangerous to humans.
Identification
The blue-ringed octopus hardly ever exceeds eight inches (20 centimeters) in size. Their most distinctive feature is the blue iridescent rings that cover their yellow-colored body; however, it is important to emphasize that this feature is only displayed when the animal is disturbed, hunting or mating. When calm or at rest, the animal may display an overall yellowish, grey or beige coloration without any visible blue rings. The blue-ringed octopus is more active at night, spending most of the day hidden in its nest in shallow areas or tide pools.
Epidemiology
Blue-ringed octopus envenomations are very rare. These animals are only endemic to southern Japan, Australia and the western Indo-Pacific. Cases outside of this region are generally due to deliberate handling of aquarium specimens. There are only a handful of reported fatal cases. Full recovery is expected with timely professional medical intervention.
Mechanism of Injury
As with all cephalopods, octopi have a strong beak similar to those of parrots and parakeets. All octopi have some sort of venom to paralyze their victims, but the blue-ringed octopus bite may contain an extremely powerful neurotoxin called tetrodotoxin (TTX), which can be up to 10,000 times more potent than cyanide and can paralyze a victim in minutes. Theoretically, a little over one-half milligram of this venom—the amount that can be placed on the head of a pin—is enough to kill an adult human. Certain bacteria present in the blue-ringed octopus’ salivary glands synthesize the toxin. TTX is not unique to the blue-ringed octopus; certain newts, dart frogs, cone snails and pufferfish can also be a source of TTX intoxication, though from different mechanisms.
Signs and Symptoms
A blue-ringed octopus bite is usually painless or no more painful than a bee sting; however, even painless bites should be taken seriously. Neurological symptoms dominate every stage of envenomation, and manifest as paresthesia (tingling and numbness) progressing to paralysis that could potentially culminate in death. If envenomation has occurred, signs and symptoms usually start within minutes and may include paresthesia of the lips and tongue. This is usually followed by excessive salivation, trouble with pronunciation (dysarthria), difficulty swallowing (dysphagia), sweating, dizziness and headache. Serious cases may progress to muscular weakness, incoordination, tremors and paralysis. Paralysis may eventually affect respiratory muscles, which can lead to severe hypoxia with cyanosis (blue or purple tissue discoloration due to insufficient oxygen in the blood).
Prevention
These animals are not aggressive, and divers should not fear blue-ringed octopi. If encountered, avoid handling these animals. Due to their small size and lack of skeleton, a blue-ringed octopus den might be a small space only accessible through a tiny crevice, so avoid picking up bottles, cans or mollusk shells in areas they inhabit.
First Aid
Care is supportive. There is no antivenom available. If someone is bitten:
Clean the wound with freshwater and provide care for a small puncture wound.
Apply the pressure immobilization technique. NOTE: TTX is a heat-stable toxin, so the application of heat will not denature the toxin.
Watch for signs and symptoms of progressive paralysis.
Be prepared to provide mechanical ventilations with a bag valve mask device or a manually triggered ventilator.
Do not wait for signs and symptoms of paralysis. Always seek an evaluation at the nearest emergency department. NOTE: The bite site might be painless and still be lethally toxic.
Wound excision is never recommended.
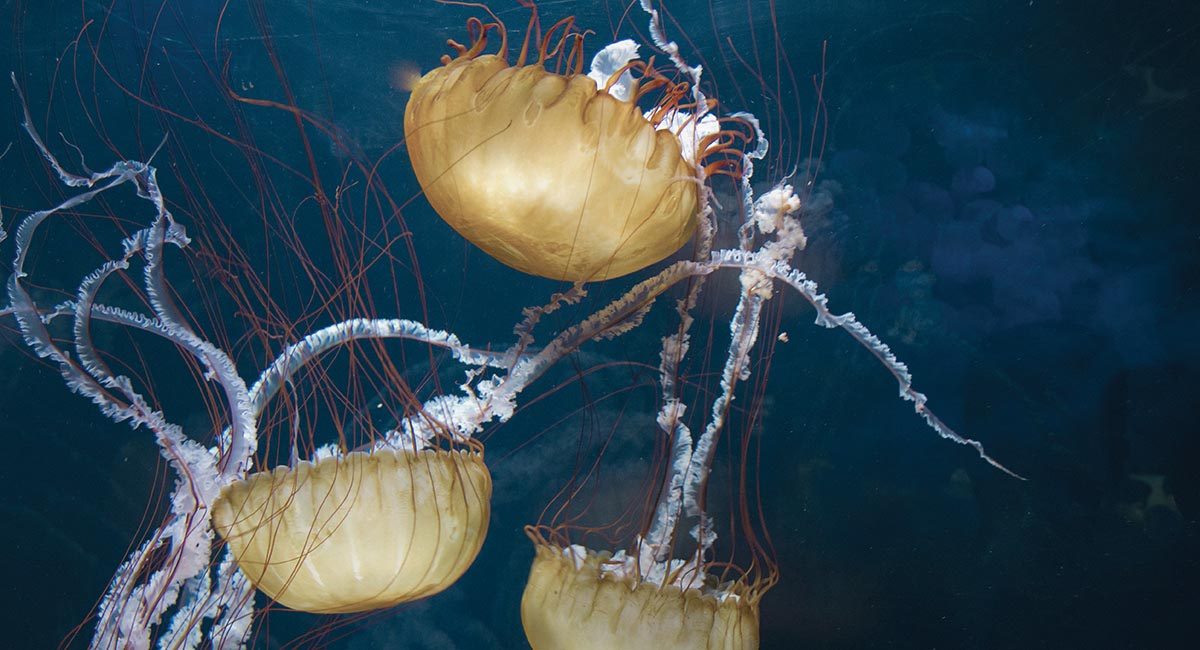
Box Jellyfish
Box jellyfish (cubozoans) are cube-shaped medusa notorious for possessing one of the most potent venoms known to mankind. Certain species can kill an adult human in as little as three minutes, scarcely enough time for any rescue response.
Biology and Identification
Medusas are the migrant form of cnidarians. In the case of box jellyfish, their bell-like body is cube shaped, with tentacles extending from each corner. Box jellyfish are complex animals with a propulsion mechanism and a relatively sophisticated nervous system for a jellyfish. They have up to 24 eyes, some of them with corneas and retinas, enabling them to not only detect light but also to see and circumnavigate objects to avoid collision.
While some jellyfish live off of symbiotic algae, box jellyfish prey on small fish, which are immediately paralyzed upon contact with their tentacles. Then the tentacles are retracted, carrying the prey into the bell for digestion. Some species hunt daily, and at night some species can be observed resting on the ocean floor.
Epidemiology and Distribution
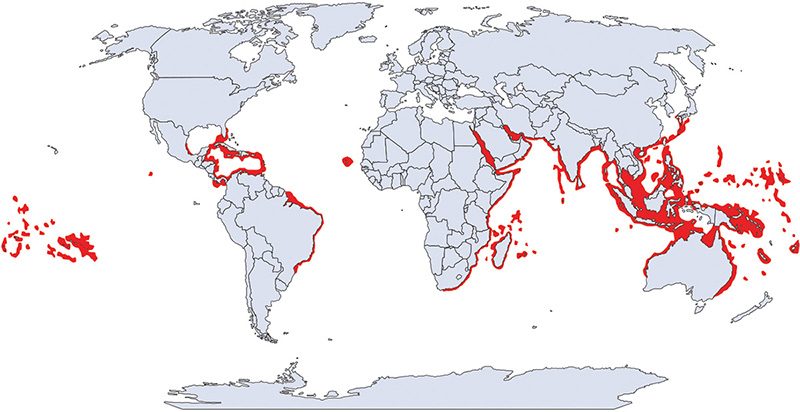
From 1884 to 1996, there were more than 60 reported fatalities from box jellyfish stings in Australia. There are species of box jellyfish in almost all tropical and subtropical seas, but life-threatening species seem to be restricted to the Indo-Pacific.
Notorious Species
SEA WASP
Found in the coastal waters of Australia and Southeast Asia, sea wasp is the common name for the most dangerous cnidarian: Chironex fleckerii. The largest cubozoan, sea wasps have a bell approximately eight inches (20 centimeters) in diameter and tentacles ranging from a few centimeters to up to 10 feet (three meters). Contact with these animals triggers the most powerful and lethal envenomation process known to science. Sea wasp envenomation causes immediate excruciating pain followed by cardiac failure. Death may occur in as little as three minutes.
Recent studies have identified a component of the venom that drills a hole in red blood cells, causing a massive release of potassium, possibly responsible for the lethal cardiovascular depression. The same study may have also identified a way to inhibit this effect, which in the coming years could prove to be clinically promising.
FOUR-HANDED BOX JELLYFISH
The four-handed box jellyfish (Chiropsalmus quadrumanus) habitat spans from South Carolina to the Caribbean, the Gulf of Mexico and as far south as Brazil. The four-handed box jellyfish can inflict extremely painful stings and is the slightly smaller American cousin to the Australian sea wasp. There is one documented case of a four-year-old boy who was stung in the Gulf of Mexico and died within 40 minutes.
BONAIRE BANDED BOX JELLYFISH
Bonaire banded box jellyfish (Tamoya ohboya) is a relatively unknown, highly venomous species found in the Dutch Caribbean. Since 1989, there have been roughly 50 confirmed sightings primarily in Bonaire with the remainder on the shores of Mexico, St. Lucia, Honduras, St. Vincent and the Grenadines. There have only been three reported cases of envenomation, which lead to intense pain and skin damage; only one case required hospitalization.
IRUKANDJI SYNDROME
Tiny box jellyfish found near Australia, Carukia barnesi and Malo kingi, are responsible for the infamous and extremely painful symptomatic complex known as Irukandji syndrome. These small cubozoans’ bells are only a few millimeters with tentacles up three feet (one meter). Fortunately, fatalities from these smaller species are rare, but stings are extremely painful and can cause systemic symptoms including cardiovascular instability that should prompt immediate medical attention. Survivors have reported a feeling of impending doom, claiming they were certain that they could not survive such intense, generalized pain; however, it is important to emphasize that a single sting should not be fatal.
Though stings from lesser-known species of cubozoans are not necessarily lethal, they can still be very painful. An immediate medical evaluation is always recommended.
Prevention
Properly research the areas you intend to dive.
Avoid known box jellyfish habitats if you are not sure the dive site or swimming area is safe. If stung, cardiovascular stability can rapidly deteriorate with very little time for any effective field intervention.
In Northern Queensland, Australia, net enclosures are placed in the water where box jellyfish are known to be during summer months (November to May), but these cannot guarantee safety.
Minimize unprotected areas. Always wear full wetsuits, hoods, boots and gloves. Something as simple as nylon pantyhose worn over the skin will prevent jellyfish stings.
Carry sufficient household vinegar with you to all dive sites.
First Aid
If stung by any jellyfish, follow these procedures in this order:
Activate local emergency medical services.
Monitor victim’s airway, breathing and circulation. Be prepared to perform CPR at any moment (particularly if you suspect box jellyfish).
Avoid rubbing the area. Box jellyfish tentacles can be cylindrical or flattened, but they are coated with cnydocites, so rubbing the area or allowing the tentacles to roll over the skin will exponentially increase the affected surface area and the envenomation process.
Apply household vinegar to the area. Generously pour or spray the area with vinegar for no less than 30 seconds to neutralize any invisible remnants. You can pour the vinegar over the area or use a spray bottle, which optimizes application. Let the vinegar stand for a few minutes before doing anything else. NOTE: This will not do anything to the pain or the venom already injected, but it is intended to stabilize any remaining unfired nematocysts on the diver’s skin before you try to remove them.
Wash the area with seawater (or saline). Use a syringe with a steady stream of water to help remove any tentacle remains. Do not rub. NOTE: Do not use freshwater; this could cause massive nematocyst discharge.
Apply heat. Immerse the affected area in hot water (upper limit of 113°F/45°C) for 30 to 90 minutes. If you are assisting a sting victim, try the water on yourself first to assess tolerable heat levels. Do not rely on the victim’s assessment, as intense pain may impair his ability to evaluate tolerable heat levels. If you cannot measure water temperature, a good rule of thumb is to use the hottest water you can tolerate without scalding. Note that different body areas have different tolerance to heat, so test the water on the same area where the diver was injured. Repeat if necessary. If hot water is not available, apply a cold pack or ice in a dry plastic bag. NOTE: Application of heat has two purposes: 1) it may mask the perception of pain; and 2) it may assist in thermolysis. Since we know the venom is a protein that has been superficially inoculated, application of heat may help by denaturing the toxin.
Always seek an emergency medical evaluation.
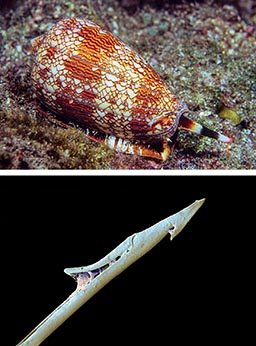
Cone Snails
Cone snails are marine gastropods characterized by a conical shell and beautiful color patterns. Cone snails possess a harpoon-like tooth capable of injecting a potent neurotoxin that can be dangerous to humans.
Identification and Distribution
There are about 600 different species of cone snails, all of which are poisonous. Cone snails live in shallow reefs partially buried under sandy sediments, rocks or corals in tropical and subtropical waters. Some species have adapted to colder waters.
Mechanism of Injury
Injuries typically occur when the animal is handled. Cone snails administer stings by extending a long flexible tube called a proboscis and then firing a venomous, harpoonlike tooth (radula).
Signs and Symptoms
A cone snail sting can cause mild to moderate pain, and the area may develop other signs of acute inflammatory reaction like redness and swelling. Conustoxins affect the nervous system and are capable of causing paralysis possibly leading to respiratory failure and death.
Epidemiology
The prevalence and incidence of cone snails envenomations is unknown, but it is probably a very rare occurrence in divers and the general population. Shell collectors (professional or amateur) may be at higher risk.
Prevention
If you see a beautiful marine snail that looks like a cone, it is probably a cone snail. It is difficult to tell whether a cone snail inhabits a given shell as they are able to hide inside them. Since all cone snails are venomous, err on the side of safety and do not touch it.
First Aid
Unfortunately, there is no specific treatment for cone snail envenomations. First aid focuses on controlling pain, but may not influence outcomes. Envenomation will not necessarily be fatal, but depending on the species, the amount of venom injected, and the victim’s size and susceptibility, complete paralysis may occur and this may lead to death. Cone snail venom is a mixture of many different substances including tetrodotoxin (TTX).
Clean the wound with freshwater and provide care for a small puncture wound.
Apply the pressure immobilization technique. NOTE: Application of heat might help with pain management, but since TTX is a heat-stable toxin, the application of heat will not denature the toxin.
Watch for signs and symptoms of progressive paralysis.
Be prepared to provide mechanical ventilations with a bag valve mask device or a manually triggered ventilator.
Do not wait for signs and symptoms of paralysis. Always seek an evaluation at the nearest emergency department. NOTE: The bite site might be painless and still be lethally toxic.
“Wash thoroughly, use soap and keep it clean and dry.”
Bites account for the majority of marine life associated trauma. Fortunately, serious encounters are extremely rare. Traumatic injuries are usually the result of an animal’s defensive reaction to a perceived threat or misidentification of a diver’s body part as a food source. Most puncture wounds do not contain venom and are, therefore, a traumatic injury. Bleeding is the most common acute complication to trauma, while infections are the most common secondary complication. In this chapter, we will cover the more common traumatic injuries, how to prevent them and how to properly manage them.
An abrasion is a superficial scrape that occurs when the skin is rubbed or bumped against a rough object.
Epidemiology
Skin abrasions, minor skin cuts and scrapes are very common among recreational divers. Accidental contact with rocks, corals, wrecks and other hard surfaces in or around dive sites can cause injury. Divers with poor buoyancy control frequently report abrasions. In addition, divers who dive close to the bottom or through narrow passageways without the protection of full-length wetsuits often report minor abrasions on their lower extremities.
Risks to Divers
Skin abrasions expose your underlying tissues to microorganisms, significantly increasing the risk of infections. Bleeding can also be of concern, particularly when the injury occurs on highly perfused areas like your face, head, hands and fingers.
Prevention
To avoid skin abrasions, you must master buoyancy control and use mechanical protection like gloves and full-body wetsuits. Though thermal insulation may not be necessary in tropical dive destinations, protection from potential skin abrasions as well as from stinging microscopic life is always a good idea. It is important to note that in an attempt to protect underwater fauna, gloves might not be permitted at some dive destinations. Ask the local dive operator about its protocols before wearing gloves; it may help to explain your reasons for wanting to wear them.
First Aid
In case of minor skin abrasions, follow these basic first aid guidelines:
Wash the area thoroughly with clean freshwater (sterile if available).
Apply antiseptic solution (iodine-based antiseptic solutions may be contraindicated in patients with hyperthyroidism).
Control bleeding by applying direct pressure with a sterile bandage.
If bleeding has been controlled:
Let the area dry out.
Apply triple antibiotic ointment.
Cover the area with a sterile bandage.
Have the wound evaluated by a medical professional within 24 hours to assess risk of infections.
If bleeding persists:
Cover the wound with clean dressings and keep them in place.
Continue to apply pressure.
Seek an immediate medical evaluation.
Treatment
For abrasions or amputations with significant bleeding, contact local emergency medical services immediately, apply bleeding control techniques and monitor the patient’s vital signs. Be prepared to manage shock.
Stingrays
Stingrays are shy, peaceful fish. They do not represent a threat to divers unless startled, stepped on or deliberately corralled and threatened. Most injuries occur in shallow waters when divers or swimmers are walking in areas where stingrays reside.
Biology and Identification
Rays are closely related to sharks: class Chondrichthyes, chondr- meaning cartilaginous and -ichthyes meaning fish. It’s important to note that not all rays have stingers. Stingrays are a specific group of rays classified in the suborder Myliobatoidei, which consists of eight families: deep water stingrays, sixgill stingrays, stingarees, round rays, butterfly rays, river stingrays, eagle rays and whiptail stingrays.
The approximate stingray wingspan varies across species from one foot to more than six feet (two meters). Some freshwater species can weigh up to 1,300 pounds (600 kilograms).
Distribution
There are species of stingrays in nearly all oceans. Some families consist of only freshwater species, which are typically found in tropical, subtropical and temperate river environments.
Mechanism of Injury
Stingrays are not aggressive by any means, and injuries are rarely fatal. The stingray’s defense mechanism consists of a serrated barb at the end of its tail with venom glands located at the base of the barb. The venom is a variable mixture of substances, none of which are specific to the animal; therefore, the creation of antivenom is not possible. Stingrays will strike when threatened or stepped on. The barb can easily tear wetsuits and penetrate skin, and may cause deep, painful lacerations.
Epidemiology
It is estimated that stingrays are responsible for approximately 1,500 accidents each year in the United States. Prevalence on other countries might be higher, particularly injuries associated with freshwater species, but epidemiological data is either elusive or inexistent.
Signs and Symptoms
Stingrays can inflict mild to severe puncture wounds or lacerations. The initial symptom is pain, which can be significant and intensify over several hours. Both puncture wounds and lacerations can damage major blood vessels causing severe, potentially life-threatening bleeding. The barb usually breaks off and may require professional surgical care.
It is common for stingray wounds to become infected despite proper care. Notable possible infections include cellulitis, myositis, fasciitis and tetanus.
Prevention
Avoid stepping in murky or low-visibility shallow waters where stingrays naturally inhabit.
Stingrays often burrow in the sand, making them difficult to see even in tropical waters.
If you are shore diving and you suspect there may be stingrays, carefully shuffle your feet while entering or exiting the water. This technique is known as the “stingray shuffle.” Stingrays are very sensitive animals, and the vibrations caused by this shuffling may scare them away.
First Aid
Clean the wound thoroughly.
Control bleeding if necessary.
Do not delay professional medical evaluation. The risk for tetanus and other serious infections must be professionally minimized.
Sea Urchins
Sea urchins are typically small, rounded spiny creatures found on shallow rocky marine coastlines. The primary hazard associated with sea urchins is contact with their spines.
Biology and Identification
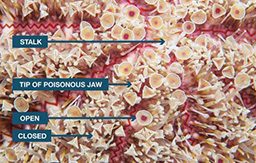
Sea urchins are echinoderms, a phylum of marine animals shared with starfish, sand dollars and sea cucumbers. Echinoderms are recognizable, because their pentaradial symmetry (they have five rays of symmetry), which is easily observed on a starfish. This symmetry corresponds with a water vascular system used for locomotion, transportation of nutrients and waste, and respiration. Sea urchins have tubular feet called pedicellariae, which enable movement. In one genus of sea urchin— the Flower Sea Urchin—some of the pedicellariae have evolved into toxic claws. In this species, the spines are short and harmless, but these toxic claws can inflict an envenomation.
Sea urchins feed on organic matter in the seabed. Their mouth is located on the base of their shell and their anus is on the top. The color of sea urchins varies depending on the species—shades of black, red, brown, green, yellow and pink are common.
Distribution
There are species of sea urchins in all oceans from tropical to arctic waters. Most human-sea urchin incidents occur in tropical and subtropical waters.
Mechanism of Injury
Sea urchins are covered in spines, which can easily penetrate divers’ boots and wetsuits, puncture the skin and break off. These spines are made of calcium carbonate, the same substance that comprises eggshells. Sea urchin spines are usually hollow and can be fragile, particularly when it comes to extracting broken spines from the skin. Injuries usually happen when people step on them on while walking across shallow rocky bottoms or tide pools. Divers and snorkelers are often injured while swimming on the surface in shallow waters as well as when entering or exiting the water from shore dives.
Epidemiology
Although little epidemiological data is available, sea urchin puncture wounds are common among divers, particularly when in shallow waters, near rocky shores or in close proximity to wrecks and other hard surfaces. The DAN Medical Information team receives at least one call a week regarding sea urchin injuries, typically from divers and snorkelers swimming in very shallow waters near rocky shores.
Signs and Symptoms
Sea urchin
Injuries are typically in the form of puncture wounds, often multiple and localized. Skin scrapes and lacerations are also possible. Puncture wounds are generally painful and associated with redness and swelling. Pain ranges from mild to severe depending on several factors, including the species, the body area of the wound, joint or muscular layers compromised, number of punctures, depth of puncture, and the individual’s threshold for pain. Multiple puncture wounds may cause limb weakness or paralysis, particularly with the long-spined species of the genus Diadema. On very rare occasions, immediate life-threatening complications may occur.
Prevention
Be observant while entering or exiting the water from shore dives, particularly when the bottom is rocky.
If swimming, snorkeling or diving in shallow waters, near rocky shores or in close proximity to wrecks and other hard surfaces, maintain a prudent distance and buoyancy control.
Avoid handling these animals.
First Aid
There is no universally accepted treatment for sea urchin puncture wounds. Both first aid and definitive care is symptomatic.
Apply heat. Immerse the affected area in hot water (upper limit of 113°F/45°C) for 30 to 90 minutes. If you are assisting a sting victim, try the water on yourself first to assess tolerable heat levels. Do not rely on the victim’s assessment, as pain may impair his ability to evaluate tolerable heat levels. If you cannot measure water temperature, a good rule of thumb is to use the hottest water you can tolerate without scalding. Note that different body areas have different tolerance to heat, so test the water on the same area where the diver was injured. Repeat if necessary. NOTE: Very few species of sea urchins contain venom. If present, hot water immersion may also help denature any superficial toxins.
Remove any superficial spines. Tweezers can be used for this purpose; however, sea urchin spines are hollow and can be very fragile when grabbed from the sides. Your bare fingers are a softer alternative to hard tweezers. NOTE: Do not attempt to remove spines embedded deeper in the skin; let those be handled by medical professionals. Deeply embedded spines may break down into smaller pieces, complicating the removal process.
Wash the area thoroughly, but avoid forceful rubbing and scrubbing if you suspect there may still be spines embedded in the skin.
Apply antiseptic solutions or over-the-counter antibiotic ointments if available.
Do not close the wound with tape or glue; this might increase the risk of infection. NOTE: Deep puncture wounds are the perfect environment to culture an infection, particularly tetanus.
Regardless of any first aid provided, always seek a professional medical evaluation.
Treatment
Contrary to popular belief, very few species of sea urchins are actually toxic. Pain and swelling is often the result of the body’s reaction to myriad different antigens present on the surface of the spines.
Spines are usually covered with strong pigments, so individual puncture wounds are often clearly visible and may cause suspicion that each puncture contains a fragment of a spine. Though this is possible, it may not necessarily be the case. It is easier to assess each individual puncture once the acute inflammatory process has started to recess.
The decision of whether or not surgical removal of retained spines is necessary is usually based on joint or muscular layer involvement, and whether there is pain with movement or signs of infection. Spines will usually encapsulate in a short time, but they may not always dissolve. A reactive granuloma is a common reaction to remaining small foreign bodies. Radiological localization, fluoroscopy or an ultrasound might be useful to avoid a blind surgical extraction that may cause further spine fracture.
The use of anti-inflammatories and physical therapy is often key for managing these injuries, particularly when they involve small joints as a prolonged inflammatory process may result in fibrosis, which may limit range of motion. If signs of infection are present, the doctor may prescribe antibiotics and a tetanus booster.
Flower Sea Urchin
The Flower Sea Urchin (Toxopneustes spp.) is the most toxic of all sea urchins. Its short spines are harmless, but its pedicellariae, which look like small flowers, are tiny claws (Toxopnueustes, meaning toxic foot). These claws contain a toxin that can cause severe pain similar to that of a jellyfish sting, faint giddiness, difficulty breathing, slurred speech, generalized weakness, and numbness of the lips, tongue and eyelids.
Seafood poisonings are illnesses caused by the ingestion of a natural toxin present in seafood. This toxicity can be inherent to the species as is the case in fugu and other tetraodontiforms, or toxicity can result from external contamination such as shellfish poisonings or ciguatera. Many gastrointestinal issues commonly attributed to seafood poisonings are often actually result of gastrointestinal infections caused by ingestion of harmful bacteria, parasites or viruses, and for that reason they are not included in this text.
In this chapter, we will discuss ichthyosarcotoxism, a form of food poisoning resulting from ingestion of fish flesh containing natural toxins. Ichthyosarcotoxism originates from the Greek words ichthyo (fish), sarx (flesh) and toxism (intoxication or poisoning). The three main ichthyosarcotoxisms are ciguatera, scombroid fish poisoning and tetrodotoxism. We will also cover shellfish-related intoxications. Since shellfish are bivalve mollusks not fish, these cases cannot be called an ichthyosarcotoxism.
Ciguatera poisoning occurs when contaminated reef fish are consumed. Specific reef fish bioaccumulate toxins produced by microorganisms in their diet. Though ciguatera intoxication should not be fatal, there is no treatment, so it is prudent to become familiar with potentially toxic species to avoid this poisoning.
Source of Intoxication
Ciguatera is caused by ingesting fish contaminated with certain toxins collectively known as ciguatoxins, which are produced by photosynthetic unicellular dinoflagellates (Gambierdiscus toxicus) that are part of phytoplankton. Dinoflagellates are epiphytes, which means they live on macro algae and dead coral surfaces. Small reef fish feed on these corals and macro algae accidentally ingesting these dinoflagellates. As these smaller fish are eaten by larger predators, the toxin is transmitted up the food chain and accumulates in the tissues of top predators through a process known as bioaccumulation. Human poisoning can potentially occur when any of the fish involved in this chain are consumed, but poisoning is much more likely when eating the larger predators.
Species known to be a source of intoxication include barracudas, snappers, moray eels, parrotfish, groupers, triggerfish and amberjacks, but other species have been known to cause occasional outbreaks. Ciguatera toxins rarely contaminate pelagic fish such as tuna, marlins, dolphinfish or other ray-finned fish. Ciguatoxin can be found around the world in the tropical reef belt between 35 degrees north latitude and 35 degrees south latitude.
Epidemiology
Ciguatera is probably the most common type of marine food poisoning. It is endemic in Australia, the Caribbean and the South Pacific islands. Ciguatera cases should be naturally limited to these areas, but due to commercial imports, cases of ciguatera have been reported in areas like St. Louis, Missouri and New York City.
Approximately 50,000 reported cases of ciguatera poisoning occur annually worldwide. Epidemiological data regarding ciguatera poisoning is challenging to collect; because of the wide array of symptoms, ciguatera is often misdiagnosed or undiagnosed. People in endemic areas often disregard medical evaluation, while imported cases probably go undiagnosed or unreported, because physicians outside of endemic regions may be unfamiliar with symptoms of a tropical toxin. Recent studies have suggested that the incidence of this illness is continuing to increase, though this might be due to increased reporting rather than an increased occurrence of the disease.
Signs and Symptoms
Toxicity depends on exposure and dose (how much is ingested). Symptom onset usually occurs two to six hours after ingestion. Symptoms can last for weeks to years, and in some cases may lead to long-term disability.
Signs and symptoms can be highly variable, but typically include neurological or gastrointestinal manifestations; about 80 percent of patients showing varying degrees of impairment in both systems. The most common manifestations include:
Gastrointestinal symptoms such as abdominal pain and gastroenteritis, nausea, vomiting or diarrhea. These initial symptoms typically resolve without intervention within a few hours.
Neurological symptoms including paresthesia (tingling and numbness), ataxia (uncoordinated muscle movements) and vertigo. Severe cases may include cold allodynia (temperature reversal), a burning sensation upon contact with cold objects. Neurological symptoms may persist and are occasionally misdiagnosed as multiple sclerosis. In patients with a recent history of diving, muscular weakness and pain, these neurological symptoms can also be confounder for decompression illness.
Skin itching that can persist for weeks and worsen as a result of activities that increase skin temperature like exercise and alcohol consumption.
Prevention
Avoid consuming fish species commonly associated with ciguatera include barracuda, grouper, snapper, parrotfish, moray eels, triggerfish and amberjacks.
Ciguatoxin is odorless, tasteless and heat-resistant—it will not taste different, and cooking will not prevent intoxication.
While the whole fish will contain toxins, the highest concentrations are typically found in the liver, intestines and gonads.
Treatment
There is no definitive treatment for ciguatera poisoning. Both first aid and hospital care is aimed at symptom control. If vomiting is profuse, it is important to correct possible dehydration. If you suspect ciguatera, you should seek a medical evaluation. There are many folk remedies, but the efficacy of these has not been studied. The best course of action is prevention through education and avoidance of seafood in endemic or suspected areas.
The term ciguatera is actually inaccurate. “Ciguatera” was coined by Don Antonio Parra in Cuba in 1787 to describe an indigestion following ingestion of a type of marine snail called “cigua” (Turbo pica). The term “cigua” was somehow transferred to an intoxication caused by the ingestion of coral reef fish.
Scombroid Fish Poisoning
Scombroid fish poisoning is a foodborne illness that results from eating spoiled fish containing high amounts of histamine.
Source of Intoxication
There are many different species of fish that can be involved in scombroid poisoning, including mackerel, tuna, bonito, albacore, sardines, anchovies, mahi-mahi, amberjacks, marlin and herrings.
If scombroids are poorly refrigerated after being caught, the fish will begin to decompose, and bacteria from the fish’s gastrointestinal tract will invade its flesh. Many fish contain a significant amount of an amino acid called histidine in their flesh. When decomposition begins, the bacteria from the gastrointestinal tract breaks histidine down into histamine (a small nitrogen compound involved in regulation of immune reactions and inflammatory responses). While ingestion of histidine is harmless, ingestion of large quantities of histamine can mimic an allergic reaction.
Epidemiology
In the United States and Europe, scombroid fish poisoning accounts for up to 40 percent of seafood-borne illness outbreaks. Between 1998 and 2002, there were 167 reported outbreaks in the United States affecting 703 persons with no fatalities. Scombroid fish poisoning can happen anywhere in the world where susceptible fish are harvested. This poisoning is more common when consuming fish caught recreationally or from small-scale operations; it rarely occurs in highly regulated fish harvests.
Signs and Symptoms
Ingestion of large quantities of histamine can mimic an allergic reaction. Symptom onset may range from minutes after consumption to up to two hours and typically resolves within 24 hours.
Symptoms may include:
Skin flushing
Oral burning
Nausea
Abdominal cramps
Diarrhea
Palpitations
Sweating
Signs may consist of:
Redness (diffuse erythema)
Elevated heart rate at rest (tachycardia)
Hypo- or hypertension
Wheezing (likely in individuals with a history of asthma, chronic obstructive pulmonary disease or reactive airway disease)
Due to its resemblance to an allergic reaction combined with poor knowledge of intoxication, scombroid fish poisoning is commonly misdiagnosed as a seafood allergy. Anyone showing signs and symptoms compatible with allergic reactions should seek an immediate medical evaluation as allergic and allergic-like reactions can be life threatening.
Prevention
Scombroid fish poisoning is entirely preventable by immediately storing fresh fish in coolers or ice containers away from direct sunlight. The Centers for Disease Control and Prevention (CDC) recommends temperatures below 40°F (4.4°C) at all points during the fish supply chain.
Affected fish may have a peppery taste, but normal taste does not guarantee safety.
Histamine is heat stable, so cooking does not prevent scombroid fish poisoning.
Treatment
As opposed to genuine allergic reactions, where the source of histamine is internal, treatment for scombroid fish poisoning does not require the use of corticosteroids or adrenaline (epinephrine). Instead, scombroid fish poisoning responds very well to oral antihistamines, typically showing positive results within 10 to 15 minutes.
Never assume oral antihistamines are enough to control a presumed scombroid fish poisoning on your own. Always seek for professional medical evaluation and let a medical doctor decide over treatment and best course of action.
Red Tide & Shellfish Poisonings
Red tide is a colloquial term for a specific phenomenon known as harmful algal bloom. Occasionally, large concentrations of aquatic microorganisms naturally bloom in coastal areas. The rapid accumulation of algal blossom can be significant enough to cause a green, red or brown discoloration of estuarine and freshwater environments.
Scientists discourage the term red tide, because these phenomena are unrelated to tidal water movements and may not necessarily be red in color or present any discoloration at all. Instead, when these algal blooms are associated with potentially harmful toxins, a more precise and favored terminology is harmful algal bloom (HAB).
Negative Impact on Ecosystems
Among the involved microorganisms certain species of phytoplankton may be present, which can produce harmful natural toxins that can become concentrated in tissues of filter feeders like shellfish and other mollusks and crustaceans. The whole food chain may be affected, and millions of fish may die as a result.
Danger to Humans
These toxins can affect commercial fisheries and represent a public health threat. People who consume contaminated shellfish may suffer a variety of shellfish poisonings, some of which are potentially lethal. Hazards related to HAB may not be limited to shellfish consumption, so avoid harvesting any type seafood on areas where HAB is known to have endemic outbreaks.
Shellfish Poisonings
Shellfish are bivalve (two-part shells) mollusks that capture nutrients by filtering water. During this process, these filter feeders can accumulate toxins and other contaminants. When humans consume these bivalves, they may be poisoned. These toxins are water-soluble and heat- and acid-stable—they are unaltered by ordinary cooking methods. Shellfish poisonings are a group of four different syndromes caused by eating bivalve mollusks contaminated with toxins produced by microscopic algae.
SYNDROMES
There are four different types of shellfish poisonings that are primarily associated with mollusks such as mussels, clams, oysters and scallops.
PARALYTIC SHELLFISH POISONING (PSP)
These mollusks can accumulate a toxin called saxitoxin, which is produced by phytoplankton (dinoflagellates, diatoms and cyanobacteria). Some shellfish remain toxic for several weeks, while others can store the toxin for up to two years.
PSP blooms are associated with harmful algal blooms, which can occur in almost all oceans. PSP can be fatal, particularly in children. Symptoms can appear a few minutes after ingestion and include nausea, vomiting, diarrhea, abdominal cramps, numbness or burning around the mouth, gums, tongue and progressing to the neck, arms, legs and toes. Other symptoms may include dry mouth, shortness of breath, slurred speech and loss of consciousness. Signs of toxicity and mortality are also seen in wild animals.
AMNESIC SHELLFISH POISONING (ASP)
This rare syndrome is caused by consuming shellfish contaminated with a toxin called domoic acid produced by certain marine diatoms.
Symptoms can appear 24 hours after ingestion of contaminated mollusks and may include nausea, vomiting, diarrhea, abdominal cramps and hemorrhagic gastritis. Neurological signs are severe and can take up to three days to develop. Neurological signs include dizziness, disorientation, visual disturbances, short-term memory loss, motor weakness, seizures, increased respiratory secretions and life-threatening dysrhythmias (irregular heartbeat). Death is rare. Resulting conditions due to permanent damage to the central nervous system may include short-term memory loss and peripheral neuropathy (weakness, numbness or pain as a result of nerve damage).
DIARRHEAL SHELLFISH POISONING (DSP)
Certain dinoflagellates produce a toxin known as okadaic acid that can cause a diarrheic syndrome. This toxin can damage the intestinal mucous membrane making it very permeable to water, which causes significant diarrhea as well as nausea, vomiting and abdominal cramps.
Symptoms can strike within a few minutes to an hour of ingesting contaminated shellfish and can last for about one day. No life-threatening symptoms have ever been recorded, but serious dehydration may occur.
NEUROTOXIC SHELLFISH POISONING (NSP)
NSP is caused by a toxin called brevetoxin, naturally produced by a dinoflagellate known as Karenia brevis. Brevetoxin can cause a variety of neurological symptoms very similar to ciguatera. NSP is generally not life threatening, but hospitalization is recommended until all other possible causes have been ruled out. In the United States and the Gulf of Mexico, a blossom of Karenia brevis usually causes the phenomena known as HAB.
Prevention
HABs occur throughout the world, killing millions of marine animals and affecting fisheries. Before harvesting your own seafood from coastal areas, research where HABs may occur and avoid consuming self-caught shellfish and fish from areas known to have HABs. Commercial fisheries tend to be safer than small scale artisanal harvesters.
The National Oceanic and Atmospheric Administration (NOAA) has a NOAA HAB (Red Tide) Watch page on Facebook. This system provides an operational forecast for harmful algal blooms. For those not on Facebook, NOAA’s Tides & Currents portal also provides an Operational Forecast System for HABs.
The Florida Fish and Wildlife Conservation Commission offers an online resource with a current map of Red Tide counts in the state of Florida.
Divers Alert Network encourages divers from all levels of certification to get first aid training so they are prepared to respond to diving injuries, including marine life injuries. The following chapter details some of the first aid techniques and treatments mentioned throughout the book including thermolysis, antivenoms and the pressure immobilization technique. However, it is important to emphasize that reading and understanding these materials is not a substitute for first aid training.
If you have not been formally trained, DAN highly recommends you find a qualified instructor. To find a First Aid for Hazardous Marine Life Injuries Instructor, visit the DAN Instructor Directory.
Thermolysis describes the use of heat to break down substances (thermo meaning temperature, and lysis meaning breakdown or destruction). This is often accomplished by immersing the affected area in hot water.
Proteins are essential organic compounds that perform a vast array of functions within living organisms. Most life forms live in temperatures below 122°F (50°C).
Above this temperature, their proteins will suffer an irreversible unfolding of their three-dimensional biomolecular structure. This process has damaging consequences to their function and is called protein denaturation. Application of heat may denature venoms that are comprised of proteins, thus eliminating their effect or reducing their potency.
Technique
The standard recommendations for toxin denaturation as a first aid measure call for immersing the affected area in hot freshwater with an upper limit of 113°F (45°C) for 30 to 90 minutes. This may work reasonably well when the toxin inoculation is skin deep, like a jellyfish sting, but will be less effective when toxins have been inoculated by means of deeper puncture wounds, as is the case of lionfish spines. Though quick reasoning could call for increasing the temperature, applying higher temperatures at skin level in an attempt to reach the desired temperature at a deeper level poses an unacceptable risk of burning the skin. In addition, vasodilatation caused by exposure to elevated temperatures may expedite the onset of absorption and of systemic effects.
Each case is unique and requires some estimation of the depth to which the venom was injected; for superficial inoculations, application of heat might be useful to manage pain and denature toxins, whereas for deeper inoculations, heat is for pain management only.
Risk Considerations
If you attempt to use thermolysis as a first aid measure, minimize the risk of local tissue damage to the injured diver by testing the water on yourself first on the same area that the diver is injured. Use the hottest temperatures you can tolerate and avoid scalding. Do not rely on the victim’s assessment, as intense pain may impair his ability to evaluate temperature tolerability.
Antivenom (Antivenin, Antivenene)
Antivenom is a biological product used in the treatment of venomous bites or stings (not to be confused with antidote). Though it is rare, recreational scuba divers might incur a venomous sting from certain marine life, such as stonefish or box jellyfish, necessitating the use of antivenom. Venomous bites, such as those from sea snakes, are even more uncommon.
What is Antivenom?
Antivenoms are blood-derived biological products developed by injecting an animal—typically a horse, goat or sheep—with sublethal doses of venom. The animal will gradually develop antibodies against the venom, which can then be extracted from its blood as a serum to be administered to humans. Like most blood-derived products, antivenoms require an unbroken cold chain (proper refrigeration from production through storage until administration).
Risks Considerations
Though generally not a concern for first responders, administering antivenoms is not free of risk. Intravenous administration of animal serums can cause anaphylactic shock in susceptible individuals.
What About Antivenom Autoinjectors?
Occasionally, DAN is asked about autoinjectors for antivenoms. Conceptually, these antivenom autoinjectors would work similarly to the way epinephrine autoinjectors (like EpiPen®) work for intramuscular administration. Though it is certainly a compelling idea, antivenoms are much more complex blood-derived products than epinephrine. As such, they have a much shorter shelf life and require an unbroken cold chain. In addition, antivenoms are administered intravenously, a skill which is beyond first aid responders. These limiting factors make this idea relatively impractical for field operation.
Pressure Immobilization Technique
The pressure immobilization technique is a first aid skill intended to contain venom within the bitten area and prevent it from moving into central circulation, where the venom could affect vital organs. The technique consists of pressure to prevent lymphatic drainage and immobilization to prevent venous return (blood flow back to the heart) caused by the pumping action of skeletal muscle.
Technique
Use an elastic bandage and splinting to administer proper pressure and immobilization. An inelastic cloth is not ideal as it is difficult to achieve optimal pressure.
Begin bandaging a few inches above the bite site (between the bite and the heart).
Wind the bandage around the limb with overlapping turns moving up the limb and then back down past the bite site.
The wrap should be tight enough to administer pressure, but you should still have normal feeling, color and a palpable pulse.
Use a splint or suitable substitute to immobilize the limb.
If possible, hold upper extremities with a sling.
The Heart & Diving
Cardiovascular health is an essential component of scuba diving safety. Cardiovascular health is an essential element of safe diving. But heart health can deteriorate gradually as divers age, and this can put divers at risk. This book covers the basic concepts of normal heart functions in physical activities, the physical fitness requirements of diving, how heart diseases may affect dive fitness, and how divers can maintain their fitness capacity.
Chapter 1: Basics of Your Heart & Circulatory System
“Nearly 1/3 of all diving fatalities are associated with an acute cardiac event.”
Scuba diving is an appealing recreational activity for people of all ages. Indeed, diving in favorable conditions requires little exertion, making it easy for the uninitiated to assume that diving is a safe and effortless pastime. But it is essential to keep in mind that during any dive, perilous conditions and circumstances can arise that may call for vigorous exercise on a moment’s notice.
Immersion alone is a stressor on the body, especially the heart and circulatory system. People who have limited exercise capacity may be pushed to their limit by diving — to the point of serious injury and even death. This chapter explains some basic information about the heart in relation to diving to help keep you safe and healthy as you dive.
How Diving Affects Your Health and Circulatory System
Scuba diving exposes you to many effects, including immersion, cold, hyperbaric gases, elevated breathing pressure, exercise and stress, as well as a postdive risk of gas bubbles circulating in your blood. Your heart’s capacity to support an elevated blood output decreases with age and with disease. Having a healthy heart is of the utmost importance to your safety while scuba diving, as well as to your ability to exercise generally and your life span. The information in this booklet is devoted to helping you understand how heart disease can affect you while you’re diving and how you can promote optimal heart health.
Effects of Immersion
Immersion in water near the temperature of the human body exposes your body to a pressure gradient, which shifts blood from the vessels in your legs to those in your chest cavity. This increases the volume of blood within your chest by up to 24 ounces (700 milliliters). Your heart thus takes in an additional 6 to 8 ounces (180 to 240 milliliters) of blood, resulting in an enlargement of all four chambers, an increase in pressure in your right atrium, a more than 30-percent increase in cardiac output and a slight increase in your overall blood pressure.
Baroreceptors (sensors that perceive a change in blood pressure) within your body’s major vessels react to all these changes by decreasing the activity of your sympathetic nervous system, which governs what’s popularly called the “fight-or-flight” response. As a result, your heart rate declines and the concentration in your plasma of norepinephrine, a hormone of the sympathetic nervous system drops; in response to the drop in norepinephrine, your kidneys excrete more sodium, and your urine production increases.
Effects of Cold
Water has high thermal conductivity—that is, your body loses more heat when you’re immersed in water than when you’re in dry air. You’ll feel more comfortable at a given air temperature than when you’re immersed in water of the same temperature. And when your body loses heat, that intensifies the narrowing of your peripheral blood vessels (a condition known as “peripheral vasoconstriction”). This in turn sends more blood to your heart, which increases the filling pressure on the right side of your heart and makes it pump more blood. Constriction of the body’s small arteries also increases the resistance to blood flowing through the periphery of your body, which raises your blood pressure, meaning your heart has to exert itself more to maintain an adequate flow of blood throughout your body.
Effects of Pressure
Breathing air under increased pressure, as you do when scuba diving, also affects your heart and circulatory system. Increased levels of oxygen cause vasoconstriction, increase your blood pressure and reduce your heart rate and heart output. And increased levels of carbon dioxide—which may accumulate in the body when you exercise during a dive, due to reduced pulmonary ventilation caused by dense gases—can increase the flow of blood through your brain, which can speed up oxygen toxicity if you’re breathing a hyperoxic gas mix (one with an elevated level of oxygen).
Effects of Exercise
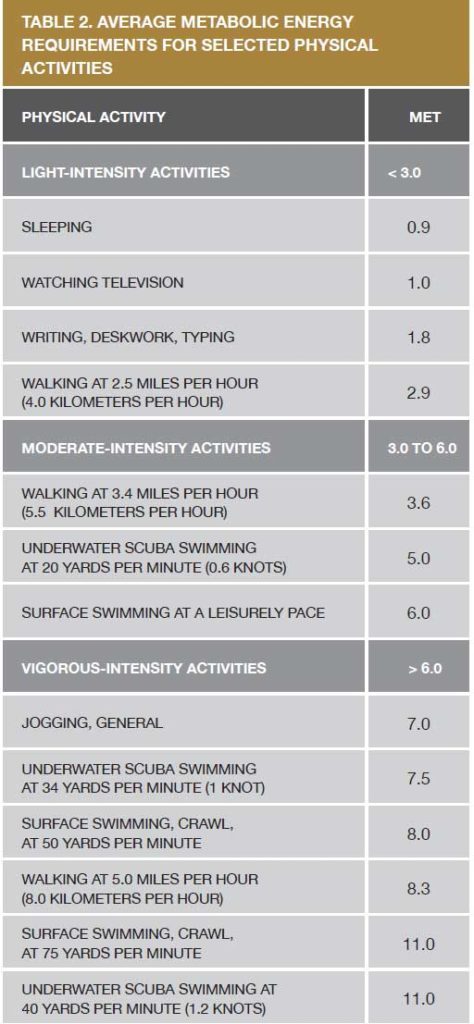
Diving can be very physically demanding, but recreational divers have the option of choosing diving conditions and activities that typically do not require a lot of exertion. Nevertheless, any dive places some metabolic energy demands on your body. For example, slow, leisurely swimming on the surface represents a moderate-intensity activity (see Table 2 on page 11), while swimming with fins on the surface requires up to 40 percent less energy than barefoot swimming. But the addition of scuba equipment increases drag on the swimmer and thus the energy cost of swimming. A 1996 paper in the journal Medicine & Science in Sports & Exercise showed that wearing just one scuba tank may increase a diver’s energy consumption by 25 percent over regular surface swimming at the same speed, and that using a drysuit may result in another 25 percent increase in energy consumption.
Most dives at neutral buoyancy and with no current require only short intervals of intermittent swimming at a slow pace and thus represent low-to-moderate intensity exercise. Exercise intensity is measured by a value known as metabolic equivalent (MET), with 1 MET representing the amount of energy consumed when at rest. (See page 11 for a detailed description of MET calculations.) It is suggested that divers be able to sustain exercise at 6 METs for a period of 20 to 30 minutes. Since people can sustain only about 50 percent of their peak exercise capacity for a protracted period, it is recommended that divers be able to pass an exercise stress test at 12 METs.
Effects of Stress
Your autonomic nervous system (ANS)—the largely involuntary system that regulates internal functions, such as your heart rate, respiratory rate and digestion—is affected by diving, too. Among the components of the ANS are the sympathetic and parasympathetic systems; while the sympathetic system governs your body’s “fight-or-flight” response, the parasympathetic system governs resting functions and helps your body conserve energy. In healthy individuals, diving generally increases parasympathetic effects, preserving the heart rate and a measure known as heart rate variability. A dive that is perceived as stressful, however, pushes the ANS in the other direction, meaning sympathetic effects prevail—resulting in an increase in the heart rate, a decline in heart rate variability and an increase in the risk of arrhythmia.
Serious Adverse Effects
Most of the effects that diving has on your heart and circulatory system fall within your body’s capacity to adapt, but sometimes serious adverse reactions can occur. A reaction known as bradyarrhythmia (a very slow and irregular heartbeat) can cause sudden death upon a diver’s entry into the water, especially in individuals with a preexisting rhythm anomaly. Conversely, tachyarrhythmia (a very rapid and irregular heartbeat) can also cause sudden death, especially in divers with structural or ischemic heart disease. And overexertion or the effects of stress may strain the heart and result in acute manifestations of previously undiagnosed ischemic heart disease.
Breath-hold diving can have particularly serious adverse cardiac effects; these effects occur in quick succession in a response known as the “diving reflex.” Its most significant elements include bradycardia (a slowing of the heart rate); the peripheral vasoconstriction reaction described above; and progressive hypoxia (or lack of an adequate supply of oxygen). To avoid bursting a lung, scuba divers must not hold their breath during ascent.
Cardiac Health and Your Risk of Death While Diving
Statistics show that about one-third of all diving fatalities are associated with an acute cardiac event. In a recent study of DAN members, the incidence of diving-related deaths overall was determined to be 16 per 100,000 divers per year, and of diving-related deaths due to cardiac causes, to be nearly a third of that number—5 per 100,000 divers per year. It is of particular note that the risk of cardiac-related death while diving is 10 times higher in divers over age 50 than in those under 50. Indeed, the study of DAN members showed a continuous increase in risk with increasing age. While some suspected cardiac events may be provoked by dive-specific activities or situations, other cardiac events may not be caused by a dive at all—inasmuch as sudden cardiac death also occurs while engaged in surface swimming or land-based sporting activities of various sorts and even while at rest or during sleep.
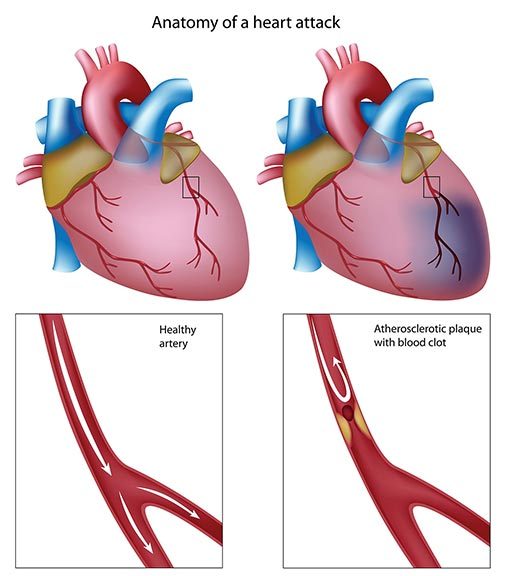
Acute myocardial infarctions (commonly known as “heart attacks”) that are brought on by exertion — such as while swimming against a current, in heavy waves or under conditions of excessive negative buoyancy — are likely involved in some dive-provoked fatalities. Heart attacks are caused by an insufficient blood supply to the muscles of the heart; diving-related heart attacks typically occur in middle-aged males with undiagnosed coronary artery disease.
Diving (or just immersion) may also provoke acute arrhythmias, or disturbances of the heart’s rhythm, that can likewise result in sudden death. Arrhythmias are more likely to cause death in older divers. As Dr. Carl Edmonds explains in his book Diving and Subaquatic Medicine, and DAN data confirms, “The victim often appeared calm just before his final collapse. Some were unusually tired or resting, having previously exerted themselves, or were being towed at the time—suggesting some degree of exhaustion. Some acted as if they did not feel well before their final collapse. Some complained of difficulty in breathing only a few seconds before the collapse, whereas others underwater signaled that they needed to buddy breathe, but rejected the offered regulator. Explanations for the dyspnea include psychogenic hyperventilation, autonomic induced breathing stimulation and pulmonary edema—the latter being demonstrated at autopsy. In all cases there was an adequate air supply available, suggesting that their dyspnea was not related to equipment problems. Some victims lost consciousness without giving any signal to their buddy, whereas others requested help in a calm manner.”
The incidence of sudden cardiac death (SCD) also increases with age. Patterns of SCD are similar among divers and among the general population; nevertheless, it is important that divers not dismiss the possibility of a causative relationship between diving and SCD. Cases of SCD where there was no obvious external provoking factor occur more frequently in older divers. Postmortem examinations of SCD victims are more likely to reveal signs of previously unsuspected heart disease than a specific precipitating event. The best way to prevent SCD is thus to prevent heart disease and to maintain physical fitness and wellness as you age.
Understanding the Concept of Aerobic Exercise Capacity
Your capacity for sustained physical activity depends on the amount of energy your body can produce in a process using oxygen called aerobic capacity. Your individual aerobic capacity depends on how well your cardiovascular system—your heart and blood vessels—works. It’s the system that moves your blood through your lungs, where it’s loaded with oxygen, and then distributes it to every part of your body, where the oxygen sustains life, nourishes your muscles and supports your ability to exercise. The “motor” of the circulatory system is the heart. The heart is a pump made of live tissue: muscles, supportive tissue and a conduction system that produces the electrical signals which stimulate your heart’s pumping action. An empty heart weighs an average of a little over half a pound (250 to 300 grams) in females and between two-thirds and three-quarters of a pound (300 to 350 grams) in males. It has four chambers: the right atrium, right ventricle, left atrium and left ventricle.
The atria receive blood at low pressure. The right atrium receives venous blood returning to the heart from all over the body after it’s been depleted of oxygen. The left atrium receives blood returning to the heart from the lungs after it’s been enriched again with oxygen. The ventricles do most of the pumping. The right ventricle pumps blood to and through the lungs, while the left ventricle maintains the circulation of blood throughout the body, to all its organs and tissues. Blood flows through the heart in only one direction, thanks to a system of valves that open and close at just the right time. How hard your heart has to work varies depending on many factors, including your activity level.
On average, a human heart pumps about 2.4 ounces (70 milliliters) of blood per heartbeat—a measure that’s known as “stroke volume.”
The heart of an individual at rest beats, on average, 72 times per minute (this is your “heart rate”), which results in a cardiac output as follows:
1.3 gallons (5 liters) of blood per minute.
1,900 gallons (7,200 liters) per day.
700,000 gallons (2,628,000 liters) per year.
48 million gallons (184 million liters) over an average life span of 70 years.
And that output is just to meet the body’s basic metabolic needs at rest: about 3.5 milliliters of oxygen per kilogram of body mass per minute. This resting metabolic rate is designated as one metabolic equivalent, which is expressed as “1 MET.” When you exercise, your body’s muscles require more oxygen, so your blood flow increases to meet that need; your heart rate may increase threefold and your stroke volume may double. This increases the cardiac output of a person of average fitness from about 1.3 gallons (5 liters) per minute to between 4 and 5 gallons (15 and 20 liters) per minute, and of a top athlete to as much as 10 gallons (40 liters) per minute. And not only does the blood flow increase, but more oxygen is extracted from each unit of blood. As a result of these changes, the metabolic level of a person of average fitness exercising at peak capacity increases to about 12 METs, and of a top athlete running a 4:17 mile (or a 22.5-kilometers-per-hour pace) may increase to 23 METs.
The Effects of Aging on Your Cardiovascular System
An individual’s ability to sustain a high level of exercise for a prolonged period of time decreases with age, even with healthy aging. This decline can be slowed by regular exercise, but it cannot be avoided completely. The decline is caused by a weakening of the functions of all the body’s systems, though the focus here is on the heart.
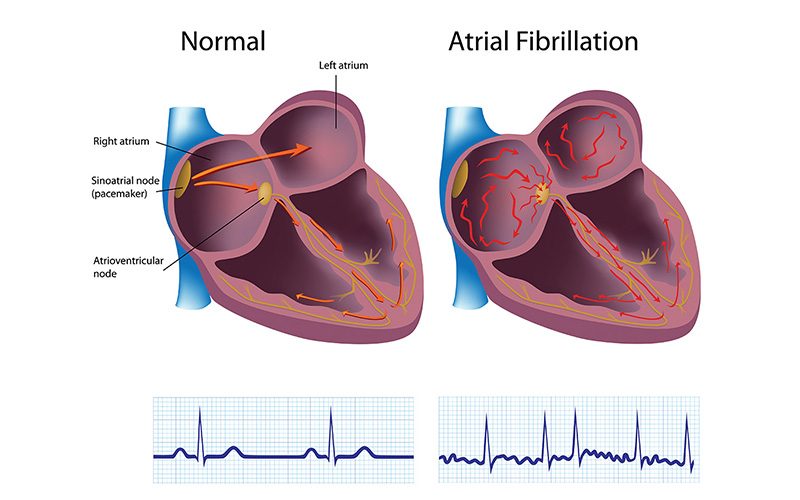
The heart has a pacing system that controls the heartbeat and regulates the electrical signals that stimulate the heart’s pumping action. Over time, this natural pacemaker loses some of its cells, and some of its electrical pathways may get damaged. These changes can result in a slightly slower heart rate at rest and a greater susceptibility to abnormal rhythms (the most common of which is known as “atrial fibrillation”).
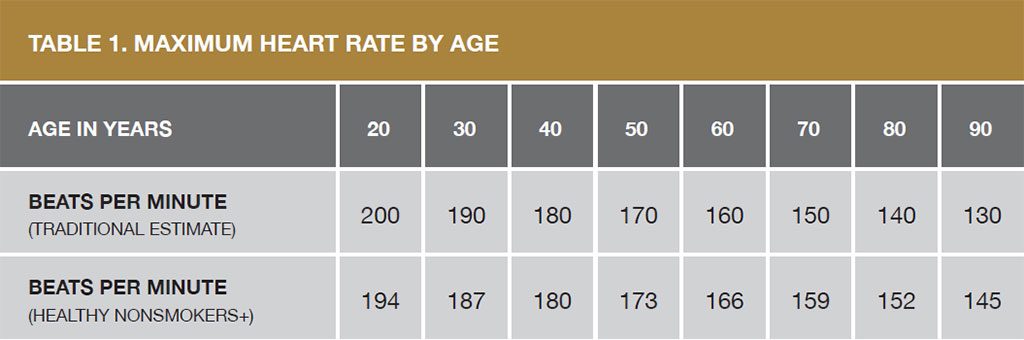
With increasing age, all the structures of the heart also become more rigid. The muscles of the left ventricle get thicker, the heart may increase slightly in size and the volume of the left ventricle may decline. As a result, the heart may both fill and empty more slowly, thus putting less blood into circulation. The increase in one’s heart rate and cardiac output in response to physical activity is also diminished, and one’s maximum heart rate declines. The drop in maximum heart rate appears to be greater than average in sedentary individuals and in those with overt cardiovascular disease.
* The traditional formula for calculating maximum heart rate, proposed in the 1970s, was 220 less the individual’s age. + Tanaka and coauthors proposed an updated formula in 2001 for healthy nonsmokers of 208 less 7/10ths of the individual’s age. Source: Modified from “Age-predicted maximal heart rate revisited” by H. Tanaka H et al. Journal of the American College of Cardiology; 2001; Vol. 37; pages 153-156
The autonomous nervous system changes with age, too. Normally, its parasympathetic component sets the level of the heart rate at rest, while its sympathetic component governs the heart in anticipation of and in response to physical activity—stimulating a timely and appropriate increase in blood flow to support the activity. Continuous adjustments between the sympathetic and parasympathetic systems result in minute variations in the heart rate (a factor known as “heart rate variability”) that are evident on a beat-to-beat basis—the kind of sensitive regulation that is a signature of a healthy control system. With increasing age, however, the contribution of the parasympathetic system wanes; the sympathetic system’s activity increases, even at rest; heart rate variability disappears; and the heart’s rhythm becomes more prone to disruption. This age-related falloff in heart rate variability and increase in resting heart rate (due to the decline in parasympathetic activity) are responsible for a 2.6-fold increased risk of SCD.
Calculating Physical Activity Intensity
The intensity of any physical activity can be calculated directly—by measuring the amount of oxygen you use for energy metabolism (a factor that’s abbreviated as VO2, short for “volume of oxygen”) per minute of exercise—or indirectly—by measuring your heart rate and using that value as an index of the strain your exertion is placing on your heart and lungs.
Direct Measurement of Exercise Intensity
The amount of energy you use at any given time is proportional to the amount of oxygen your body requires. At rest, the average healthy person uses roughly 3.5 milliliters of oxygen per kilogram of body weight per minute; this is known as “resting metabolic rate.” The energy cost of a physical activity can be expressed as a multiple of resting metabolic rate; this is known as “metabolic equivalent of task,” or simply metabolic equivalent, and is abbreviated as MET.
An individual of average fitness can achieve about a 12-fold increase in metabolic rate (which is expressed as “12 METs”), while top athletes can exceed a 20-MET increase.
The table to the right lists examples of activities classified as being of light, moderate or vigorous intensity, based on the amount of energy required to do them.
Sources: “Compendium of physical activities: an update of activity codes and MET intensities”; “Oxygen consumption in underwater swimming”; and “Oxygen uptake studies of divers when fin swimming with maximum effort at depths of 6–176 feet” (see the list of further readings on page 53 for details on these sources).
An individual’s peak aerobic capacity is expressed as maximum oxygen uptake while engaged in all-out exercise (which is abbreviated as “VO2 max”). Measuring VO2 max accurately requires following strict protocols in a sports-performance lab – a procedure known as a “maximal exercise test.” Conducting such tests is time-consuming and expensive, so they are used only in special situations.
Indirect Estimation of Exercise Intensity
It is also possible to make a relative estimate of an activity’s intensity by measuring its effects on your heart rate and respiration rate. This can be done in several ways.
Talk test: If an average healthy person can talk but not sing while exercising, that activity is considered to be of moderate intensity. A person engaged in vigorous-intensity activity is not able to say more than a few words without pausing for a breath. If you must gasp for air and cannot talk during what is generally considered to be moderate-intensity exercise, it means that your physical capacity is below average.
Heart rate test: Your heart rate rises in a regular fashion as the intensity of your activity increases (though the maximum heart rate you’re able to achieve will decline as you age). You can figure the average maximum heart rate for healthy individuals your age by subtracting your age from 220. For example, the maximum heart rate for a 50-year-old would be calculated as follows: 220 – 50 = 170 beats per minute (bpm). You can then use your actual heart rate to estimate the relative intensity of various activities you engage in and to indirectly estimate your maximum exercise capacity. Experts often recommend reaching and sustaining a certain heart rate to improve or maintain fitness.
Submaximal exercise test: A submaximal exercise test can be used to figure your maximum exercise capacity without exceeding 85 percent of the estimated maximum heart rate for your age. Conducting such a test calls for gradually increasing your exercise intensity, based on a defined protocol, while your heart rate is being monitored. When you reach the target heart rate, you stop exercising and your maximum exercise capacity can then be extrapolated using various methods. However, because of variations in the relationship between heart rate and exercise intensity due to age, fitness level and other factors, an indirect estimation of maximum aerobic capacity has limited value. Nevertheless, the test is still a valuable clinical tool to assess an individual’s tolerance for exercise and likelihood of having ischemic heart disease.
Physical Activity Recommendations
Adults need two types of regular activity to maintain or improve their health—aerobics and strength training. The Centers for Disease Control and Prevention’s 2008 Physical Activity Guidelines for Americans recommends at least two and a half hours a week of moderate-intensity aerobic exercise to achieve health benefits, and five hours a week to achieve additional fitness benefits. And just as important as engaging in aerobic exercise is doing muscle-strengthening activities at least two days a week.
Physical activities are commonly classified by intensity into one of the following four categories:
SEDENTARY BEHAVIOR: Sedentary behavior refers to activities that do not substantially increase one’s heart rate or energy expenditure above the resting level; included in this category are activities like sleeping, sitting, lying down and watching television. Such activities involve an energy expenditure of 1.0 to 1.5 METs.
LIGHT-INTENSITY PHYSICAL ACTIVITY: Light physical activity—which is often grouped with sedentary behavior but is, in fact, a distinct activity level—involves an energy expenditure of between 1.6 and 2.9 METs and raises the heart rate to less than 50 percent of one’s maximum heart rate. It encompasses such activities as slow walking, deskwork, cooking and washing dishes.
MODERATE-INTENSITY PHYSICAL ACTIVITY: Physical activity that increases the heart rate to between 50 percent and 70 percent of one’s maximum heart rate is considered to be of moderate intensity. For example, 50-year-olds have an estimated maximum heart rate of 170 beats per minute (bpm), so the 50-percent and 70-percent levels would be 85 bpm and 119 bpm. That means a moderate intensity activity for 50-year-olds is one that keeps their heart rate between 85 bpm and 119 bpm. By contrast, 30-year-olds have an estimated maximum heart rate of 190 bpm, making a moderate-intensity activity one that raises their heart rate to between 95 bpm and 133 bpm.
VIGOROUS-INTENSITY PHYSICAL ACTIVITY: A vigorous-intensity activity is one that increases the heart rate to between 70 percent and 85 percent of one’s maximum heart rate. For 60-year-olds, that would be between 122 bpm and 136 bpm; for 25-year-olds, it would be between 136 bpm and 167 bpm.
Engaging in physical activity is beneficial for one’s health, but making the transition from a sedentary lifestyle to being physically active, or increasing one’s accustomed level of activity, may be associated with increased risk—especially in individuals with preexisting heart disease. Scuba diving typically involves moderate intensity physical activity, but situations can occur that require high-intensity activity. In addition, scuba diving challenges the cardiovascular system in a variety of ways that may be life-threatening for individuals with heart disease or a low capacity for exercise.
A common pre-activity screening tool is the Recreational Scuba Training Council (RSTC) Medical Statement and Guidelines. The RSTC questionnaire asks about your medical history, as well as symptoms and signs of chronic and acute diseases. If prospective divers have any of the listed conditions, they are advised to consult with a physician to obtain a medical evaluation of their fitness to dive. Most dive operators use the RSTC form to screen customers, and if you check any conditions that call for medical evaluation but cannot present documentation of a recent exam that has cleared you for diving, you may be unable to dive. So you should complete the RSTC Medical Statement in advance of any trip during which you plan to dive and, if necessary, obtain a written evaluation from a physician knowledgeable about diving medicine—and take it with you on your trip.
And remember that it is of the utmost importance that you be honest in filling out the questionnaire: You hold the keys to your safe participation in any physical activity, including scuba diving.
In addition, regardless of their medical condition, men age 45 and older and women age 50 and older are advised to review their health annually with their primary-care physician. And all divers with any risk factors for cardiac disease should see their primary-care physician before engaging in diving and should be sure to follow any advice they’re given.
Placing the Risks and Benefits of Physical Activity in Perspective
In general, engaging in regular physical activity reduces an individual’s risk of death due to heart disease—but in susceptible individuals, vigorous activity can increase the risk of an acute myocardial infarction (heart attack) or of sudden cardiac death (SCD). Individuals with advanced atherosclerosis—a disorder that involves a narrowing of the arteries due to a buildup of fatty deposits on their inner walls—are especially susceptible to such risks.
The incidence of both acute myocardial infarction and SCD is greatest in generally sedentary individuals, especially those who engage in unaccustomed physical activity. A paper published in the New England Journal of Medicine found that habitually sedentary men were 56 times more likely to experience cardiac death during or after vigorous exercise than when at rest; by contrast, very physically active men were only five times more likely to die during or after vigorous exercise than when at rest. Another New England Journal of Medicine paper reported that an acute myocardial infarction was 50 times more likely during or soon after vigorous physical exercise in the least active than in the most active subjects.
So while sedentary individuals are advised to change their lifestyle and take up regular physical exercise—starting with low-intensity activities and gradually increasing the intensity at which they exercise—they may require pre-activity screening. Individuals with any health limitations need both medical clearance and, preferably, a professional fitness coach. Individuals identified as being at high risk for cardiac problems should abstain from certain activities. For relevant guidelines, read “When to consult a health-care provider before engaging in physical activities.”
It is important to emphasize, however, that even the most restrictive practices will never be able to completely prevent cardiovascular events associated with exercise. It is thus essential that individuals who exercise recognize and report the symptoms that often precede a cardiac event; these are known as “prodromal symptoms” and may include one or more of the following:
Chest pain (known as “angina”).
Increasing fatigue.
Indigestion, heartburn or other gastrointestinal symptoms.
Excessive breathlessness.
Ear or neck pain.
A feeling of vague malaise.
Upper respiratory tract infections.
Dizziness, palpitations or a severe headache.
Such symptoms have been shown to be present in 50 percent of joggers, 75 percent of squash players, 81 percent of distance runners and 60 percent of scuba divers who die while exercising. People who exercise must be aware of these facts, and physicians should query patients during medical exams about their exercise habits and their knowledge of prodromal symptoms. Divers who experience any of the symptoms above during exercise should obtain a medical evaluation before they resume diving.
“Heart disease develops 7 to 10 years later in women than in men.”
Ischemia is a term meaning that an inadequate supply of blood is reaching a part of the body. Ischemic heart disease thus means not enough blood is getting to the heart muscle. It is almost always caused by atherosclerosis (a narrowing of the arteries due to fatty deposits on their inner walls) in the coronary arteries (the arteries that supply the heart muscle), and it is the most common cause of heart disease. The prevalence of ischemia increases with age. The first manifestation of ischemic heart disease is sometimes a fatal heart attack, but the condition’s presence may be signaled by symptoms that should prompt lifesaving actions. Knowing these symptoms can mean living longer. And preventing heart disease in general means living happier — without symptoms or functional limitations.
Atherosclerosis is popularly referred to as “hardening of the arteries.” It’s the result of cholesterol and other fatty material being deposited along the inner walls of the arteries. The condition has different manifestations, depending on which arteries are affected; it causes coronary artery disease (CAD) in the heart, cerebrovascular atherosclerosis in the brain and peripheral artery disease (PAD) in the limbs.
The walls of the arteries, in response to the deposition of fatty material, also thicken. The result is a progressive reduction in the flow of blood through the affected vessels. These effects are especially damaging in the heart; CAD is the leading cause of death in the United States and other industrialized countries.
Many factors contribute to the development of atherosclerosis, including a diet high in fat and cholesterol, smoking, hypertension, increasing age and a family history of the condition. Women of reproductive age are generally at lower risk of atherosclerosis due to the protective effects of estrogen.
Medications typically used to treat atherosclerosis include nitroglycerin (which is also used in the treatment of angina, or chest pain) and calcium channel blockers and beta blockers (which are also used in the treatment of high blood pressure, or hypertension; see “Antihypertensives” for more on these drugs). Sometimes, individuals with CAD may need what’s known as a revascularization procedure, to re-establish the blood supply — typically a coronary artery bypass graft or angioplasty. If such a procedure is successful, the individual may be able to return to diving after a period of healing and a thorough cardiovascular evaluation (see “Issues Involving Coronary Artery Bypass Grafts.”).
Effect on Diving
Symptomatic coronary artery disease is not consistent with safe diving: don’t dive if you have CAD. The condition results in a decreased delivery of blood — and therefore oxygen — to the muscular tissue of the heart. Exercise increases the heart’s need for oxygen. Depriving your heart of oxygen can lead to abnormal heart rhythms and/or myocardial infarction, (a heart attack). The classic symptom of CAD is chest pain, especially following exertion. But unfortunately, many people have no symptoms before they experience a heart attack.
A history of stroke — or of “mini strokes” known as transient ischemic attacks (TIAs) — are also, in most cases, not consistent with safe diving.
Cardiovascular disease is a significant cause of death among divers. Older divers and those with significant risk factors for coronary artery disease should have regular medical evaluations and undergo appropriate screening studies, such as a treadmill stress test.
Myocardial Infarction
When any of the arteries supplying the heart become blocked, a myocardial infarction, or heart attack, will occur if the blockage (or “infarct”) is not eliminated quickly. The heart muscle supplied by that artery then becomes starved for oxygen and eventually dies. If the infarct is large enough, the heart’s ability to pump blood is compromised, and circulation to all the body’s other critical organs is affected. The heart’s electrical system may also be adversely affected, resulting in an abnormal rhythm known as ventricular fibrillation.
The main cause of myocardial infarction is coronary artery disease (CAD), or a gradual narrowing of the arteries that supply the heart with blood. Eventually, a piece of the fatty plaques affixed to the arteries’ inner walls may break free and lodge in a smaller vessel, resulting in total occlusion. CAD affects 3 million Americans and kills more than 700,000 each year; it is the most common life-threatening disease. A blockage that results in a myocardial infarction can also be caused by a bubble of gas or a clot within a blood vessel. But, simply stated, whatever the cause of the occlusion, it means the oxygen required by the heart muscle can no longer be supplied through the blocked vessel.
The classic symptoms of myocardial infarction include radiating chest pain (angina) or pain in the jaw or left arm. Other symptoms include heart palpitations; dizziness; indigestion; nausea; sweating; cold, clammy skin; and shortness of breath.
If a myocardial infarction is suspected, it is essential that emergency medical care be called and the affected individual evacuated to a hospital. In the meantime, keep the individual calm and administer oxygen. At the hospital, the treatment options include conservative medical management, anticoagulation drugs, heart catheterization or stenting or even coronary artery bypass surgery.
Preventing myocardial infarction calls for addressing any risk factors, such as obesity, diabetes, hypertension or smoking. A healthy diet and regular exercise are also important preventatives.
Effect on Diving
Anyone with active ischemic CAD should not dive. The physiologic changes involved in diving, as well as the exercise and stress of a dive, may initiate a cascade of events leading to a myocardial infarction or to unconsciousness or sudden cardiac arrest while in the water. Divers who have been treated and evaluated by a cardiologist may choose to continue diving on a case-by-case basis; essential aspects of such an evaluation include the individual’s exercise capacity and any evidence of ischemia while exercising, of arrhythmias or of injury to the heart muscle.
Coronary Artery Bypass Grafts
A coronary artery bypass is the surgical correction of a blockage in a coronary artery; it is accomplished by attaching (or “grafting”) onto the damaged vessel a piece of a vein or artery from elsewhere in the body, so as to circumvent the blockage.
Doctors perform this procedure many hundreds of times a day, all around the country — more than half a million times a year. If a bypass is successful, the individual should be free of the symptoms of coronary artery disease, and the heart muscle should once again receive a normal supply of blood and thus oxygen.
A blocked coronary artery can also be treated with a less invasive procedure, coronary angioplasty. It consists of inserting a catheter with a tiny balloon on its tip into the area of the blockage, then inflating the balloon to open the artery. This procedure does not require opening the chest and can be performed in an outpatient setting.
Effect on Diving
Individuals who have had a coronary artery bypass graft or coronary angioplasty may have suffered significant cardiac damage prior to having surgery. Their postoperative cardiac function is what determines their fitness for a return to diving.
In particular, those who have had open-chest surgery need to have a thorough medical evaluation prior to diving again. After a period of stabilization and healing (6 to 12 months is the usual recommendation), such individuals should have a complete cardiovascular evaluation before being cleared to dive. They should be free of chest pain and have a normal tolerance for exercise, as evidenced by a normal stress EKG test (at 13 METs, as described in “Calculating Physical Activity Intensity”). If there is any doubt about the success of the procedure, or how open the coronary arteries are, the individual should refrain from diving.
Issues Particular to Women
Heart disease is the leading cause of death in women, and myocardial infarction (heart attack) is the leading cause of their hospitalization. The characteristics of the disease in women may differ from those in men; the age of onset, presence of risk factors, probability of aggressive diagnosis and even likelihood of appropriate treatment vary in men and women.
For example, heart disease develops 7 to 10 years later in women than in men (possibly because of the protective effect of estrogen). Myocardial infarction is less frequent in young women than in young men, but young women who have a heart attack are at greater risk of dying within 28 days of their attack. The common risk factors for heart disease have a similar predictive value for men and women; however, men more frequently have smoking as a risk factor, whereas women more frequently have hypertension, diabetes, hyperlipidemia or angina. Although women typically smoke less than men, the relative risk for myocardial infarction in women who do smoke is 1.5 to 2 times greater than in men who smoke, especially in those less than 55 years old. A higher prevalence of diabetes also contributes to higher mortality rates from heart attacks among women.
Women receive fewer advanced diagnostic tests such as coronary angiography and fewer interventions such as coronary artery bypass grafts. These differentials may be due to the fact that acute heart attacks are likely to occur at an older age in women, or to the presence of other associated diseases, but could also be due to delays in admitting women to the hospital.
The symptoms of a heart attack in women are usually the same as those in men, with chest pain (angina) being the leading symptom. However, women are more likely to attribute their symptoms to acid reflux, the flu or normal aging. In addition, the chest pain that women experience does not necessarily occur in the center of the chest or the left arm; instead, women may feel pressure in their upper back — a sensation of squeezing or as if a rope is tied around them.
Although 90 percent of women who suffer a heart attack later admit that they intuitively knew that was the cause of their symptoms, at the time they often discount them, attribute them to something else, take an aspirin or just delay calling 911. This decreases the opportunity to preserve their heart from damage and lowers their chance of survival.
These are the most common symptoms of a heart attack in women:
Uncomfortable pressure, squeezing, fullness or pain in the center of the chest; it lasts more than a few minutes or goes away and comes back
Pain or discomfort in one or both arms, the back, neck, jaw or stomach
Shortness of breath, with or without chest discomfort
Other signs, such as breaking out in a cold sweat, nausea or lightheadedness
As with men, women’s most common heart attack symptom is chest pain or discomfort — but women are somewhat more likely than men to experience some of the other common symptoms, particularly shortness of breath, nausea/vomiting or back or jaw pain.
“By 2050, it is estimated that atrial fibrillation (AFib) will affect between 5.6 million and 12 million Americans.”
The electrical wiring of your heart — which controls the rate at which your heart beats, every minute, hour and day, 365 days a year — is one of the most sophisticated and enduring pieces of nature’s engineering. However, there are some irregularities that can occur in that wiring as well as damage that can be caused by disease, all of which can cause symptoms and increase the risk of premature death. Divers, and any physicians who treat them, should be familiar with arrhythmias and their effects on the safety of scuba divers.
The term “arrhythmia” (or, sometimes, “dysrhythmia”) means an abnormal heartbeat. It is used to describe manifestations ranging from benign, harmless conditions to severe, life-threatening disturbances of the heart’s rhythm.
A normal heart beats between 60 and 100 times a minute. In well-trained athletes, or even select nonathletic individuals, the heart may beat at rest as slowly as 40 to 50 times a minute. Even entirely healthy, normal individuals experience occasional extra beats or minor changes in their heart’s rhythm. These can be caused by drugs (such as caffeine) or stress or can occur for no apparent reason. Arrhythmias become serious only when they are prolonged or when they do not result in proper contraction of the heart.
Physiologically significant extra heartbeats may originate in the upper chambers of the heart (this is called “supraventricular tachycardia”) or in the lower chambers of the heart (this is called “ventricular tachycardia”). The cause of these extra beats may be a short circuit or an extra conduction pathway in the heart’s wiring, or it may be the result of some other cardiac disorder. People who have episodes or periods of rapid heartbeat are at risk of losing consciousness during such events. Other people have a fairly stable arrhythmia (such as “fixed atrial fibrillation”) but in conjunction with additional cardiovascular disorders or other health problems that exacerbate the effect of their rhythm disturbance. A too-slow heartbeat (or a heart blockage) may cause symptoms, too.
Effect on Diving
Serious arrhythmias, such as ventricular tachycardia and many types of atrial arrhythmia, are incompatible with diving. The risk for any person who develops an arrhythmia during a dive is, of course, losing consciousness while underwater. Supraventricular tachycardia, for example, is unpredictable in its onset and may even be triggered simply by immersing one’s face in cold water. Anyone who has had more than one episode of this type of arrhythmia should not dive.
Most arrhythmias that require medication also disqualify the affected individual from safe diving. Exceptions may be made on a case-by-case basis in consultation with a cardiologist and a diving medical officer.
An individual who has any cardiac arrhythmia needs a complete medical evaluation by a cardiologist prior to engaging in diving. In some cases, electrophysiologic studies can identify an abnormal conduction pathway, and the problem can be corrected. Recently, clinicians and researchers have determined that people with some arrhythmias (such as certain types of Wolff-Parkinson-White syndrome, which is characterized by an extra electrical pathyway) may safely participate in diving after a thorough evaluation by a cardiologist. Also, in select cases, people with stable atrial arrhythmias (such as uncomplicated atrial fibrillation) may dive safely if a cardiologist determines that they have no other significant health problems.
Syncope
Syncope is an abrupt loss of consciousness followed by a relatively quick recovery. The causes of syncope range from relatively benign to life-threatening. It is seldom overlooked and usually precipitates a visit to a medical professional.
Syncope that occurs in or around the water poses particular challenges. Drowning often results when a diver loses consciousness and remains in the water. A rapid response is required to bring an unconscious diver to the surface and prevent death. Syncope can also occur upon exiting the water, due to such factors as exertion, dehydration and normal return of blood volume to the lower extremities.
The initial response to syncope should focus on the ABCs of basic life support: airway, breathing and circulation. Advanced cardiac life support may be called for. Often, placing syncopal patients flat on their back in a cool environment will quickly restore them to consciousness. If syncope occurs following a dive, it is important to consider decompression sickness, pulmonary overinflation and immersion pulmonary edema in addition to the usual causes of the condition. Although both syncope and cardiac arrest result in a loss of consciousness, they can usually be clearly differentiated.
The list of possible causes of syncope is extensive, but a good medical history can help eliminate the majority of them. The patient’s age, heart rate, family history, medical conditions and medications are key in identifying the cause. If syncope is accompanied by convulsions (known as “tonic-clonic movements”), it may have been precipitated by a seizure. If it occurs upon exertion, a serious cardiac condition may be preventing the heart from keeping up with the demands of the physical activity; chest pain may be associated with this type of syncope. If standing up quickly results in syncope, that points to a cause known as “orthostatic hypotension.” And pain, fear, urination, defecation, eating, coughing or swallowing may cause a variation of the condition known as “reflex syncope.”
A medical evaluation after an incident of syncope should include a thorough history and physical — plus interviews with witnesses who observed the individual’s collapse and who can accurately relay the sequence of events. A few cases may require more extensive investigation, and some result in no conclusion.
Effect on Diving
While a medical evaluation is being conducted, it is recommended that the affected individual refrain from any further diving. The cause of a given syncopal episode can be elusive but must be pursued — especially if the individual hopes to return to diving. Once the underlying factors have been determined, a diving medical officer and appropriate specialists should consider whether diving can be resumed safely.
Extrasystole
Heart beats that occur outside the heart’s regular rhythm are known as “extrasystoles.” They often arise in the ventricles, in which case they are referred to as “premature ventricular contractions” or sometimes “premature ventricular complexes,” abbreviated as PVCs. The cause of such extra beats can be benign or can result from serious underlying heart disease.
PVCs are common even in healthy individuals; they have been recorded in 75 percent of those who undergo prolonged cardiac monitoring (for at least 24 hours, that is). The incidence of PVCs also increases with age; they have been recorded in more than 5 percent of individuals more than 40 years old who undergo an electrocardiogram (or ECG, a test that typically takes less than 10 minutes to administer). Men seem to be affected more than women.
The extrasystole itself is usually not felt. It is followed by a pause — a skipped beat — as the heart’s electrical system resets itself. The contraction following the pause is usually more forceful than normal, and this beat is frequently perceived as a palpitation — an unusually rapid or intense beat. If extrasystoles are either sustained or combined with other rhythm abnormalities, affected individuals may also experience dizziness or lightheadedness. Heart palpitations and the sensation of missed or skipped beats are the most common complaints of those who seek medical care for extrasystole.
A medical examination of the condition begins with a history and physical and should also include an ECG and various laboratory tests, including the levels of electrolytes (such as sodium, potassium and chloride) in the blood. In some cases, doctors may recommend an echocardiogram (an ultrasound examination of the heart), a stress test and/or the use of a Holter monitor (a device that records the heart’s electrical activity continuously for a 24- to 48-hour period). Holter monitoring may uncover PVCs that are unifocal — that is, they originate from a single location. Of greater concern are multifocal PVCs — those that arise from multiple locations — as well as those that exhibit specific patterns known R-on-T phenomenon, bigeminy and trigeminy.
If serious structural disorders, such as coronary artery disease or cardiomyopathy (a weakening of the heart muscle), can be ruled out — and the patient remains asymptomatic — the only “treatment” required may be reassurance. But for symptomatic patients, the course is less clear, as there is controversy regarding the effectiveness of the available treatment options. Two drugs commonly used to treat high blood pressure — beta blockers and calcium channel blockers — have been used in patients with extrasystole with some success. Antiarrhythmics have also been prescribed for extrasystole but have met with mixed reviews. A procedure known as cardiac ablation may be an option for symptomatic patients, if the location where their extra beats arise can be identified; the procedure involves threading tiny electrodes into the heart via catheters, then zapping the affected locations to rewire the heart’s faulty circuits.
Effect on Diving
Although PVCs are present in a large percentage of otherwise normal individuals, they have been shown to increase mortality over time. If PVCs are detected, it is important that they be investigated and that known associated conditions be ruled out. Divers who experience PVCs and who are found to also have coronary artery disease or cardiomyopathy will put themselves at significant risk if they continue to dive. Divers diagnosed with R-on-T phenomenon, nonsustained runs of ventricular tachycardia or multifocal PVCs should likewise refrain from diving. Divers who experience PVCs but remain asymptomatic may be able to consider a return to diving; such individuals should discuss with their cardiologist their medical findings, their desire to continue diving and their clear understanding of the risks involved.
Atrial Fibrillation
Atrial fibrillation (AF or AFib), the most common form of arrhythmia, is characterized by a fast and irregular heartbeat. It results from a disturbance of the electrical signals that normally make the heart contract in a controlled rhythm. Instead, chaotic and rapid impulses cause uncoordinated atrial filling and ventricle pumping action. This leads to a decrease in overall cardiac output, which can affect one’s exercise capacity or even result in unconsciousness. In addition, AF causes blood to pool in the atria, which promotes the formation of blood clots that may break loose and enter the circulatory system; if this occurs, it may result in a stroke.
Recent U.S. studies have shown a rising incidence of AF overall as well as significant racial differences in its prevalence. The lifetime risk of AF (at 80 years of age) was recently found to be 21 percent in white men and 17 percent in white women but only 11 percent in African-Americans of both sexes. By 2050, it is estimated that AF will affect between 5.6 million and 12 million Americans. These figures are significant, because AF is associated with a fourfold to fivefold higher risk of ischemic stroke. Individuals with AF, after adjustment for other risk factors, also have a twofold higher risk of dementia.
The most common causes of AF are hypertension and coronary artery disease. Additional causes include a history of valvular disorders, hypertrophic cardiomyopathy (a thickening of the heart’s muscle), deep vein thrombosis (DVT), pulmonary embolism, obesity, hyperthyroidism (also called “overactive thyroid”), heavy alcohol consumption, an imbalance of electrolytes in the blood, cardiac surgery and heart failure.
Some people with AF experience no symptoms and are unaware they have the condition until it’s discovered during a physical examination. Others may experience symptoms such as the following:
Palpitations (a racing, uncomfortable, irregular heartbeat or a flip-flopping sensation in the chest)
Weakness
Reduced ability to exercise
Fatigue
Lightheadedness
Dizziness
Confusion
Shortness of breath
Chest pain
The occurrence and duration of atrial fibrillation usually falls into one of three patterns:
Occasional (or “paroxysmal”): The rhythm disturbance and its symptoms come and go, lasting for a few minutes to a few hours, and then stop on their own. Such events may occur a couple of times a year, and their frequency typically increases over time.
Persistent: The heart’s rhythm doesn’t go back to normal on its own, and treatment — such as an electrical shock or medication — is required to restore a normal rhythm.
Permanent: The heart’s rhythm can’t be restored to normal. Treatment may be required to control the heart rate, and medication may be prescribed to prevent the formation of blood clots.
Any new case of AF should be investigated and its cause determined. An investigation may include a physical exam; an electrocardiogram; a measurement of electrolyte levels, including magnesium; a thyroid-hormone test; an echocardiogram; a complete blood count; and/or a chest X-ray.
Treating the underlying cause of AF can help control the fibrillation. Various medications, including beta blockers, may help regulate the heart rate. A procedure known as cardioversion — which can be performed with either a mild electrical shock or medication — may prompt the heart to revert to a normal rhythm; before cardioversion is attempted, it is essential to ensure that a clot has not formed in the atrium. Cardiac ablation, which is described in the “Extrasystole” section, may also be used to treat AF. In addition, anticoagulant drugs are often prescribed for individuals with AF to prevent the formation clots and thus reduce their risk of stroke. It is also of note that the neurological effects of an embolic stroke associated with AF can sometimes be confused with the symptoms of decompression sickness.
Effect on Diving
A thorough medical examination should be conducted to identify the underlying cause of the atrial fibrillation. It is often the underlying cause that is of most concern regarding fitness to dive. But even atrial fibrillation itself can have a significant impact on cardiac output and therefore on maximum exercise capacity. Individuals who experience recurrent episodes of symptomatic AF should refrain from further diving. The medications often used to control atrial fibrillation can present their own problems, by causing other arrhythmias and/or impairing the individual’s exercise capacity. It is essential that anyone diagnosed with AF have a detailed discussion with a cardiologist before resuming diving.
Sudden Cardiac Arrest
Sudden cardiac arrest (SCA) — a cessation of the heart’s beating action, with little or no warning — is an acute medical emergency. During the arrest, blood stops circulating to the body’s vital organs, including the brain, the kidneys and the heart itself. Cut off from oxygen, these organs die within minutes. If the arrest is not corrected quickly, the affected individual will not survive.
The causes of SCA include myocardial infarction (heart attack), heart failure, drowning, coronary artery disease, electrolyte abnormalities, drugs, abnormalities in the heart’s electrical conduction system, cardiomyopathy (a weakening of the heart muscle) and embolism (a clot that has lodged in a major vessel).
SCA accounts for 450,000 deaths in the United States each year and for 63 percent of cardiac deaths in Americans more than 35 years old. The risk of sudden cardiac death in adults increases as much as sixfold with increasing age, paralleling the rising incidence of ischemic heart disease. The risk of SCA is greater in those with structural heart diseases, but in 50 percent of sudden cardiac deaths the victim had no awareness of having heart disease, and in 20 percent of autopsies conducted following such deaths, no structural cardiovascular abnormalities were found.
Though there is typically little warning before a sudden cardiac arrest, occasionally the individual may experience lightheadedness, difficulty breathing, palpitations or chest pain.
Immediate treatment should be focused on restoring circulation quickly using chest compressions or CPR and defibrillation. Following resuscitation, the victim should be transported to a hospital as soon as possible. Subsequent treatment may consist of efforts to eliminate the underlying cause of the arrest through administration of medication, surgery or the use of implanted electrical devices.
Preventive strategies include learning to recognize the warning signs of SCA, in case they occur; identifying, eliminating or controlling any risk factors that may affect you; and scheduling regular physical exams, as well as appropriate testing, when it is indicated.
Effect on Diving
Divers with any symptoms of cardiovascular disease should be evaluated by a cardiologist and a dive-medicine specialist regarding their continued participation in diving. In asymptomatic individuals, the risk of SCA may be evaluated by using known cardiovascular risk factors such as smoking, high blood pressure, high cholesterol, diabetes, lack of exercise and overweight. For example, people who smoke have two and a half times the risk of suffering sudden cardiac death than do nonsmokers.
Issues Involving Implanted Pacemakers
A pacemaker is a small battery-operated device that helps an individual’s heart beat in a regular rhythm. It does this by generating a slight electrical current that stimulates the heart to beat. The device is implanted under the skin of the chest, just below the collarbone, and is hooked up to heart with tiny wires that are threaded into the organ through its major vessels. In some individuals, the heart may need only intermittent help from the pacemaker, if the pause between two beats becomes too long. In others, however, the heart may depend completely on the pacemaker for regular stimulation of its beating action.
Chest with the pace maker on x-rays
Effect on Diving
Every case involving a pacemaker must be evaluated individually. The two most important factors to take into account are the following:
Why is the individual dependent on a pacemaker?
Is the individual’s pacemaker rated to perform at depths (in other words, pressures) compatible with recreational diving — plus an added margin of safety?
The reason for the second factor is that a pacemaker is implanted in tissues just under the skin and thus is exposed during a dive to the same ambient pressures as the diver. For safe diving, a pacemaker must be rated to perform at a depth of at least 130 feet (40 meters) and must also operate satisfactorily during conditions of relatively rapid pressure changes, such as would be experienced during ascent and descent.
As with any medication or medical device, the underlying problem that led to the implantation of the pacemaker is the most significant factor in determining someone’s fitness to dive. The need to have a pacemaker implanted usually indicates a serious disturbance in the heart’s own conduction system.
If the disturbance arose from structural damage to the heart muscle itself, as is often the case when someone suffers a major heart attack, the individual may lack the cardiovascular fitness to dive safely.
Some individuals, however, depend on a pacemaker not because the heart muscle has been damaged but simply because the area that generates the impulses which make the heart muscle contract does not function consistently or adequately. Or the circuitry that conducts the impulses to the heart muscle may be faulty, resulting in improper or irregular signals. Without the assistance of a pacemaker, such individuals might suffer episodes of syncope (fainting). Others may have suffered a heart attack mild enough that they sustained minimal residual damage to their heart muscle, but their conduction system remains unreliable and thus needs a boost from a pacemaker.
If a cardiologist determines that an individual’s level of cardiovascular fitness is sufficient for safe diving, and the individual’s pacemaker is rated to function at a pressure of at least 130 feet (40 meters), that individual may be considered fit for recreational diving. But once again, it cannot be emphasized strongly enough that any divers with cardiac issues check with their doctor before diving.
“The risk of a DVT occurring on a flight lasting more than four hours is between 1 in 4,650 flights and 1 in 6,000 flights.”
Your lungs have many functions in your body beyond just oxygenating your blood. One of their other important roles is filtering the venous blood that returns from the body. The venous system is characterized by slower blood flow than the arterial system, which contributes to the occasional formation of a blood clot (known as a “peripheral venous thrombosis”), which could be transported into the lungs and could even cause a pulmonary embolism (or blockage in the vessels of the lungs).
Deep vein thrombosis (DVT) is a condition in which a blood clot (a “thrombus”) forms in one or more of the body’s deep veins, usually in the legs. If a clot breaks free and travels through the circulatory system, it can lead to life-threatening conditions. For example, if a clot lodges in the lungs, it is known as a pulmonary embolism (PE) and affects the lungs’ ability to oxygenate the blood (see “Pulmonary Embolism”). Collectively, DVT and PE are sometimes referred to as venous thromboembolisms (VTEs).
A clot that originates as a DVT can also cause a stroke in individuals with a patent foramen ovale (PFO, a hole in the wall between the atria — see “Patent Foramen Ovale” for details about this condition); in such a case, the clot travels through the veins to the right atrium of the heart, passes through the PFO to the left atrium and then travels through the arteries to the brain.
DVT is not related to diving, but divers often travel, and travel is a significant risk factor for DVT. In about half of all cases of DVT, the individual experiences no noticeable symptoms before the onset of the condition. Most often, it starts in the calf. Symptoms may include the following:
Swelling in the affected leg, ankle or foot
Pain in the calf that spreads to the ankle or foot
Warmth in the affected area
A change in the color of the skin — to pale, red or blue
Most VTEs related to air travel occur within two weeks of the flight and are resolved within eight weeks. If untreated, a DVT that starts in the calf will spread up into the thigh and pelvis in about 25 percent of cases. An untreated DVT of the thigh and pelvis has about a 50 percent risk of leading to a PE, which is the most serious complication of DVT. Many cases of DVT are asymptomatic and resolve spontaneously. However, DVT often recurs in an individual who has had one episode of the condition.
Most DVTs occur in individuals with pre-existing risk factors for DVT who remain motionless for a long time — such as when traveling a long distance by plane, car or train; when doing deskwork over a period of many hours; or when bedridden. This is because immobility slows down the blood flow in the veins (a condition known as “venous stasis”); in addition, pressure on the calf from an inadequate seat can injure the vein walls. If you sit still for 90 minutes, the blood flow in your calf drops by half, and that doubles your chance of developing a blood clot. For every additional hour you spend sitting, your risk of a blood clot increases by 10 percent.
The incidence of DVT in the general population is one-tenth of one percent, but it is higher in those who have risk factors and those who travel often. Long-distance air travel may double or even quadruple the risk of suffering a VTE. Although DVT is often called the “economy class disease,” business-class travelers are susceptible, too. The risk of a DVT occurring on a flight lasting more than four hours is between 1 in 4,650 flights and 1 in 6,000 flights; this is lower than the risk in the general population, but that’s because people who take long trips are likely to be healthier than average. The incidence of DVT among travelers with a low to intermediate pre-existing risk for VTE who take a journey longer than eight hours was found to be 0.3 percent for symptomatic cases and 0.5 percent when including asymptomatic cases as well.
Risk factors for DVT include the following:
Older age (the risk rises after age 40)
Obesity (defined as a body mass index greater than 30)
Estrogen use (either hormonal contraceptives or hormone replacement therapy)
Pregnancy (including the postpartum period)
Thrombophilia (an abnormally increased tendency of the blood to clot)
Previous VTE or a family history of VTE
Active cancer
Serious medical illness
Recent surgery, hospitalization or trauma
Limited mobility
Central venous catheterization (the presence of a catheter in one’s chest, for use in administering medication or nutrients and/or drawing blood samples)
Between 75 percent and 99 percent of those who develop a travel-related VTE had more than one of these risk factors.
Height is also a factor in one’s risk of developing a travel-related DVT. People who are either very short — less than 5 feet, 3 inches (1.6 meters) — or very tall — more than 6 feet, 3 inches (1.9 meters) — appear to be at increased risk as a result of their inability to adjust their seats sufficiently to accommodate their height. In addition to effects of immobility, shorter passengers may suffer greater than usual seat-edge pressure on the backs of their knees, and taller passengers may be cramped due to insufficient leg room. All of these factors can contribute to injury of deep veins, venous stasis and activation of the blood’s clotting mechanisms.
Those who are at increased risk of DVT should wear compression socks whenever they fly or drive long distances and should consult their primary-care provider regarding the possible benefit of taking a clot-preventative such as aspirin. Although the risk of DVT for healthy people is small, everybody should be aware of the factors that can precipitate the condition — and avoid long periods of immobility. The best way to prevent DVT is to get up and walk around from time to time. It also helps to flex your feet and calf muscles regularly if you must remain seated for any length of time. Finally, it is also helpful in preventing DVT to stay well hydrated.
Effect on Diving
Any individual who has been diagnosed with acute DVT or who is taking anticoagulants should refrain from diving. It may be possible to return to safe diving after having a DVT, but the evaluation of fitness to dive must be made on an individual basis.
Pulmonary Embolism
A pulmonary embolism (PE) is an obstruction (or “embolus”) that lodges in the vasculature of the pulmonary system, or lungs. The embolus may be air, fat or a blood clot (or “thrombus”). If a PE is caused by a thrombus, the clot typically originated in the deep vein system of the legs — a condition known as deep vein thrombosis (DVT); see “Deep Vein Thrombosis” for a discussion of DVT. The resulting obstruction in the flow of blood to the lungs typically causes a drop in cardiac output and a significant drop in blood pressure.
The onset of PE can be acute or chronic. Acute PE often causes symptoms evident to the individual, while chronic-onset PE frequently reveals its presence only with very subtle findings that went unnoticed by the affected individual. An untreated PE has a high mortality rate. An especially grim prognosis applies to individuals who have a concurrent DVT, right ventricular thrombus or right ventricular dysfunction. An estimated 1.5 percent of all deaths are diagnosed as being due to PE.
Risk factors for DVT — and thus for PE — include recent surgery; a stroke; a diagnosis of autoimmune disease, malignancy or heart disease; obesity; smoking; hypertension; and a previous DVT.
Symptoms of PE include chest pain (also known as “dyspnea”), pain or swelling of the calf (signaling a DVT), hypotension (abnormally low blood pressure), an altered level of consciousness and syncope (fainting). Distension of the neck veins in the absence of other conditions — such as pneumothorax (a buildup of air in the membrane surrounding the lungs, sometimes referred to as a collapsed lung) or heart failure — may also be observed in individuals suffering a PE.
PE should be one of the first conditions considered when attempting to make a diagnosis in someone exhibiting acute onset of any of the symptoms listed above and any of the associated risk factors. Appropriate diagnostic tests may include measurement of the individual’s levels of a hormone called brain natriuretic peptide (BNP) and of a protein known as cardiac troponin, as well as a CT angiogram of the lungs.
Treatment should focus initially on managing the significant cardiopulmonary impairments that are usually involved in a PE. Such care may include breathing support from an artificial ventilator and fluid management. The use of anticoagulant medication is also important, both to treat the embolus and to stop the development of another thrombus. Thrombolysis (known as “clot-busting”), embolectomy (surgical removal of the embolus) or the placement in the vena cava (one of the large vessels in the chest) of a filter designed to prevent any future clots from reaching the lungs may also be considered — especially in anyone who goes into shock, because mortality in such cases approaches 50 percent. Similar measures may be called for in cases of PE caused by a venous gas bubble. Hyperbaric oxygen therapy may be indicated as well, if the individual’s condition does not improve or deteriorates even after the application of supportive measures.
Effect on Diving
Despite many medical advances, five-year all-cause mortality in individuals who have suffered a PE due to underlying risk factors remains more than 30 percent. And pulmonary hypertension — elevated pressure in the arteries that carry blood from the heart to the lungs, a condition that limits one’s exercise capacity — often persists in individuals who have had a PE, even after successful treatment. Thus any determination of fitness for diving by those who have had a PE must include an evaluation of their lung function, underlying conditions, anticoagulation status, exercise capacity and cardiac status.
Immersion Pulmonary Edema
Immersion pulmonary edema (IPE) is a form of pulmonary edema — an accumulation of fluid in the tissues of the lungs — that specifically affects divers and swimmers. Immersion at depth is a key factor in the development of IPE. That’s because immersion in an upright position causes a significant shift of fluid from the peripheral to the central circulatory system, resulting in higher pressure in the capillaries of the pulmonary system. Elements of the diving milieu that contribute to IPE’s occurrence include the fact that divers breathe gases that are denser than air at sea level, which means more negative pressure within chest is needed to inhale; the likelihood of gas bubbles becoming trapped in the vasculature of the lungs; the cold underwater environment; and the potential in underwater settings for exertion or panic, which can exacerbate elevated capillary pressure.
Maintaining a proper fluid balance in your lung tissue and its vasculature requires a dynamic combination of various opposing forces. Unopposed changes in any of these forces can result in a buildup of excess fluid — or edema — in your pulmonary tissue. The main variables involved in regulating this fluid balance are the following:
Oncotic pressure (a form of pressure exerted by proteins) in the pulmonary capillaries, the tiniest vessels of the circulatory system
Oncotic pressure in the pulmonary system’s interstitial fluid (fluid in the cavities of your lung tissue)
Permeability of the pulmonary capillaries
Hydrostatic pressure (the pressure of a fluid at rest) in the pulmonary capillaries
Hydraulic pressure (the pressure of a fluid that is being compressed or pumped) in the interstitial fluid
Pressure in the alveoli, the tiny air sacs of the lungs.
These factors, which collectively are known as “Starling forces,” can all be quantified and placed in an equation that can then be used to calculate the net differential of the forces.
Pulmonary edema is caused by changes in these forces — such as a drop in the levels of key proteins in the blood; leakage from the pulmonary capillaries due to sepsis (a life-threatening complication of infections); an increase in hydrostatic pressure in the pulmonary capillaries due to heart failure; and negative pressure in the alveoli due to resistance from breathing through a faulty regulator. Additional issues that can contribute to the development of pulmonary edema include side effects of some cardiovascular drugs; ARDS (acute respiratory distress syndrome, a life-threatening condition that prevents oxygen from getting to the lungs); reperfusion (a procedure that restores circulation after a heart attack or stroke); cardiomyopathy (a weakening of the heart muscle); high-altitude pulmonary edema; a pulmonary embolus (a blood clot lodged in a vessel in the lungs); re-expansion (the reinflation of a collapsed lung); pulmonary hypertension (elevated pressure in the arteries that carry blood from the heart to the lungs); lung cancer; hemorrhage (uncontrolled bleeding); and various disorders of the nervous system. Other factors can include overhydration by well-intentioned divers who have heard the conventional wisdom that dehydration is a risk factor for decompression sickness, as well as poor physical conditioning, which can result in increased negative pressure in the alveoli during deep inspiration.
The symptoms of IPE include chest pain; dyspnea (discomfort or difficulty breathing); wheezing; and pink, frothy sputum while submerged or shortly after emerging from the water. Most people who suffer an episode of IPE had no significant history or signs that would indicate a susceptibility to the condition; nevertheless, the risk of IPE does rise with age, obesity and elevated blood pressure.
Once pulmonary edema occurs, hypoxia (lack of an adequate supply of oxygen) leads to constriction of the pulmonary vasculature, which worsens the cascade of ill effects. The situation can be further aggravated by the accompanying dyspnea, which, when experienced underwater, can induce panic and uncontrolled ascent to the surface — leading to overinflation of the lungs and even near-drowning.
To help differentiate immersion pulmonary edema from other conditions with similar symptoms (such as near-drowning, pulmonary decompression sickness and pulmonary overinflation syndrome), it is important to keep in mind that IPE’s onset can occur either at depth or upon reaching the surface. And it is not necessarily precipitated by aggressive diving, a rapid ascent or the aspiration of water.
Treatment for IPE should begin with removal of the affected individual from the water (to relieve the compression of the vessels in the lower extremities, allowing centrally pooled fluids to return to the extremities) and with administration of oxygen (beginning at 100 percent and later at a reduced concentration). A diuretic such as Lasix may help to reduce excess intravascular fluid, although diuresis — the body’s natural excretion of fluid — may already be under way as a result of hormonal influences. The condition usually resolves quickly in a healthy diver. Prolonged hospitalization is rarely required; if it is necessary, it’s usually due to contributing factors, such as an underlying cardiac problem.
Effect on Diving
Some divers have one episode of IPE and never experience the condition again, but repeated episodes are likely. Any individuals who suffer a first episode of IPE are advised to undergo a detailed examination to rule out any medical conditions that may have caused the edema and then to have a thorough discussion with their physician regarding the risks of continuing to dive. And all divers are urged to have regular maintenance on their regulators, to refrain from overhydration and to attend to proper dive planning in order to avoid exertion and panic — as well as to keep conditions such as obesity and hypertension under control.