I’m a dive instructor, and I occasionally have student divers who wonder if they need to follow the flying-after-diving recommendations after just being in the pool.
Flying or travel to altitude after diving is a consideration for many divers, so it is great that the question is being asked. Fortunately, a typical shallow, low-workload, pool-diving exposure would be of minimal concern, particularly when the time is split between the bottom and the surface and the cumulative total underwater time is modest. This is a great opportunity, however, to reinforce an understanding of dive tables.
You can reference the U.S. Navy Diving Manual (USN 2008) for this guidance. An actual bottom time (the time from leaving the surface to the point of direct ascent to a stop depth or the surface) of 61-88 minutes at 15 feet of seawater (fsw) would put a diver in repetitive group C (Table 9-7). C is the maximum repetitive group allowed for immediate exposure to an altitude of 8,000 feet (Table 9-6). A maximum depth of 10 fsw would require an actual bottom time of 102-158 minutes to put a diver in repetitive group C.
Any delay between exiting the water and travel to altitude would provide an additional safety buffer as the diver offgases. Conversely, deeper dive depths, high underwater workloads and/or travel to higher altitudes would require greater conservatism.
Practically speaking, a 60-minute pool session in a 10- to 12-foot-deep pool would offer little concern for typical pressurized aircraft cabin altitudes (usually 6,000-8,000 feet altitude equivalent) or unpressurized flight or driving to a similar actual altitude. Following the flying-after-diving guidelines recommended for recreational diving would not be necessary for this (or lesser) exposure.
For completeness, the flying-after-diving guidelines for recreational diving call for a minimum 12-hour surface interval (SI) after single no-decompression dives, an 18-hour SI after multiple dives per day or multiple consecutive days of diving, and a “substantially longer” than 18-hour SI after decompression dives (Sheffield and Vann 2004). The “substantially longer” text was used to acknowledge the fact that we did not have sufficient data for precise recommendations, but it is a common rule of thumb that a 24-hour SI is desirable for decompression dives.
The DAN® flying-after-diving guidelines are applied to the altitude range of 2,000-8,000 feet. Exposures to altitudes below this range are ignored, and exposures to greater altitudes are not recommended after diving until all excess inert gas is eliminated. In comparison, the U.S. Navy uses 1,000 feet as the threshold for altitude exposure. An interesting fact is that the U.S. Navy tables rely on most of the same data used to generate the DAN guidelines. The specific guidance for different exposure profiles is primarily based on mathematical manipulation of the same data, not additional experimental data.
— Neal W. Pollock, Ph.D.
References
- Sheffield P, Vann RD, eds. DAN Flying After Diving Workshop Proceedings. Durham, NC: Divers Alert Network, 2004.
- U.S. Navy Diving Manual, Volume 2, Revision 6. NAVSEA 0910-LP-106-0957. Washington, DC: Naval Sea Systems Command, 2008: Chapter 9.
I have noticed that beginning scuba divers often get nosebleeds after dives. What causes them?
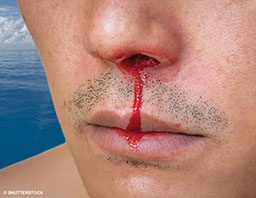
Divers, especially new divers, sometimes report nosebleeds after diving primarily because they are unaware of the importance of equalizing the sinuses and middle ears. The barotrauma that results when the sinuses are not equalized can cause blood vessels in the lining of the nose to burst. These vessels lie very close to the mucous membranes that line the nose and sinuses, and the blood can come from either of these linings. This type of barotrauma, generally the result of air being trapped within the sinuses, is not always painful, though the presence of blood can be disconcerting. With this type of injury, blood can also run down the back of the throat or pool in the sinus below the eye and emerge later. It can also act as a growth medium for bacteria and lead to sinus infections.
Individuals with a history of sinus trouble, allergies, a broken nose or a deviated septum as well as divers who currently have a cold may find equalization difficult and may experience problems with nosebleeds. It’s always best to not dive with a cold, congestion or any other condition that might block the sinus passages.
We suggest a slow, gentle descent with frequent equalizing to help decrease the risk of sinus barotrauma. Divers who are unable to equalize their sinuses or have frequent nosebleeds when scuba diving should see their personal physician or a specialist in ear, nose and throat (ENT) care for evaluation.
— Dan Nord, EMT-P, CHT
Is there any reason cold water might increase the likelihood of lung squeeze while freediving? I have experienced lung squeeze a few times, but only in cold water (around 45°F). I was shallower than 100 feet. In warm water I can reach 165 feet, so I believe the squeeze is somehow related to the water temperature.
You described your condition as lung squeeze, but it sounds like your question is really about what might have caused you to cough up blood from your lungs (presumably) under the conditions you describe. Given the variable impact of depth on the development of the condition, you could be experiencing a form of immersion pulmonary edema (IPE).

IPE is a multifactorial condition, largely a net effect of increased central blood volume, pressures within the chest and, for compressed-gas divers, increased breathing resistance. The squeeze is a primary component, but only part of the story. Immersion produces a shift in blood from the periphery to the core, and this effect can be magnified in cold water or partially replicated by wearing a tight wetsuit. Excessive fluid intake (hyperhydration) increases the risk. For compressed-gas divers, respiratory loading (most important, the effort to inhale) increases with water immersion, with breathing through a mouthpiece that adds resistance (particularly as gas density increases) and with exertion. Using compressed gas or freediving, if the net effect of the various stressors is a sufficient increase in the pulmonary artery pressure, capillary stress failure can produce a shift of blood into the lungs. Symptoms of IPE can include the perception of strain or stiffness in breathing, coughing and the coughing up of small amounts of blood.
While I cannot confirm that this is what you are experiencing, it may be that the central blood volume increase magnified by the cold water is the stressor that takes you over the edge that you skirt in warmer water exposures. IPE is most likely to appear when multiple predisposing factors are acting in concert. You may have found your own threshold.
I encourage you to consult with your medical monitors, keeping in mind that the classic squeeze is not the only risk that freedivers face.
— Neal W. Pollock, Ph.D.
A From the Medical Line article in a previous issue of Alert Diver (Summer 2015) addressed the topic of the new generation of anticoagulant medications. It mentioned that there was no way to reverse the effects of these newer anticoagulants. I recently heard this is no longer true. Can you verify this?
Indeed, a new medication called idarucizumab (Praxbind®) can reverse the anticoagulant effects of dabigatran etexilate (Pradaxa®). Reversal medications for other next-generation anticoagulants are still in development. Note that when traveling outside the U.S., however, idarucizumab may not be available in an emergency. This should prompt consideration when planning diving activities.
— Marty McCafferty, EMT-P, DMT
| © Alert Diver — Q1 2017 |