For much of the past century a small number of algorithms have been used to estimate divers’ decompression obligations. Advances in recent decades, however, have produced an array of mathematical models used in personal dive computers. All current computer models base their assessments almost exclusively on the pressure-time profile of a dive. While this is certainly the most important element of decompression sickness (DCS) risk and can provide excellent guidance, many factors influence the totality of inert gas uptake and elimination — and ultimately decompression safety. Divers can reduce their risk by thinking beyond the current algorithms 1.
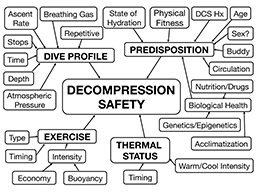
The variables affecting decompression stress can be clustered into four broad categories: dive profile, exercise profile, thermal profile and predisposition factors (Figure 1).
Dive Profile
Even for situations in which all other factors work against decompression safety, if the dive profile does not generate significant decompression stress, DCS will not develop. Critical elements of the profile include time spent at each depth, ascent rate, stop depth(s), stop duration(s) and breathing gas(es) used. Recent previous dives can alter the impact of these variables. Subtler effects are created by the water density, whether it is fresh or salt, and the atmospheric pressure at the surface. The lower the atmospheric pressure is at the surface, the greater the decompression stress for a given dive. While the greatest reduction in atmospheric pressure comes with increasing altitude, fluctuating weather conditions also have a minor effect.

Most algorithms used in dive computers provide adequate protection for typical recreational exposures, but DCS can develop even in people who dive within the limits of decompression models. The risk results from the complex interplay of the dive profile, thermal and exercise states and a host of individual factors. For some, the level of risk associated with current decompression algorithms is acceptable. Others may desire additional buffers to address differences in susceptibility or risk tolerance. Gradient factors offer one useful option for altering conservatism.
Exercise
The timing and intensity of exercise can have substantial influence on decompression safety. In the broadest sense, exercise during the descent and bottom phases of a dive promotes circulation and increases inert gas uptake, effectively increasing decompression stress. Conversely, light to moderate exercise during the ascent and stop phases will increase circulation and promote safe inert gas elimination, thus reducing decompression stress. Problematically, though, higher-intensity exertion during the ascent and stop phases or soon after the dive can promote bubble formation and increase the effective decompression stress. The best prepared divers will have the equipment and skill to control the amount of exercise needed before, during and after diving.
Exercise intensity should be kept as low as possible during the descent and bottom phases. Light exercise — on the order of no more than two to three times resting effort (2.0-3.0 metabolic equivalents [MET]) and with very low forces on the joints — is appropriate during the upper ascent and stop phases to help increase the rate of inert gas elimination. High-intensity exercise and exercise involving high joint forces should be avoided before and after dives. If undesirable physical activity is required, dive profiles should be made conservative to compensate for the increased risk.
Thermal Status
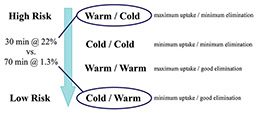
The thermal status of a diver can also have substantial influence on decompression status. A study by the U.S. Navy provides an elegant example. Dives were divided into two phases: descent and bottom, and ascent and stop 2. The water temperature was kept constant in a given phase to produce “warm” or “cold” (more accurately, “cool”) status. Dives were carried out with the phases matched (“warm/warm” and “cold/cold”) and mismatched (“warm/cold” and “cold/warm”) with divers exercising throughout. The greatest differences in DCS were evident between “warm/cold” and “cold/warm” exposures (Figure 2). The “warm/cold” condition yielded a DCS rate of 22 percent. The “cold/warm” condition was extended to more than twice the bottom time and still yielded a DCS rate of only 1.3 percent. Even if the effects of this study are exaggerated by a prolonged ascent/stop phase that allowed for bottom-time changes, the results document a dramatic impact by the timing of thermal status variations.
Diver thermal status — not water temperature, a potentially very different thing — will almost certainly be measured in the future, but meaningful monitoring will require new devices and much research data to adjust algorithms appropriately.
Maintaining a neutral thermal status during the descent and bottom phases — certainly avoiding unnecessary overheating — and trying to achieve a mild warm status without high-intensity exercise during ascent will reduce the risk of DCS. The difficulty comes in reconciling optimal practices for decompression safety with divers’ desires and normal practices. Pouring warm water into wetsuits predive or placing chemical hot packs inside suits is being replaced by active heating garments available for both wetsuits and drysuits. The problem with these strategies is that they increase inert gas uptake early in the dive when uptake is already typically highest. Since warm water and chemical hot packs lose their effectiveness over time, and active heating systems can weaken or fail, the warm-cool pattern associated with the greatest risk of DCS can develop.
Active heating garments can have legitimate value but should be used thoughtfully. Warming should never be greater than is needed, and divers should consider a low or off setting early in the dive and a gradual increase in warming during ascent. Caution is required in increasing active heating during ascent since gas solubility decreases in tissues as they warm, potentially promoting bubble formation before blood perfusion increases sufficiently to remove the gas.
Divers must also be aware that postdive warming can increase DCS risk. Taking a hot shower or getting into a hot tub will decrease the tissue solubility for inert gas and can promote bubble formation.
Ultimately, divers need adequate warmth to preserve clear thinking and physical performance, but they should be mindful of the decompression hazards created by thermal manipulation. For many divers passive systems are adequate to maintain physical and cognitive performance. Those who need or desire active warming systems should be aware that those systems can increase decompression stress even if they work correctly and that they may substantially increase decompression stress if they fail.
Predisposition
Predisposition is a catch-all category that includes an array of personal factors that can influence decompression stress. The impact of each may range from negligible to substantial for a given individual and/or dive. None of these parameters can currently be quantified sufficiently to incorporate into decompression algorithms. Understanding the potential impact, however, can help divers manage their true risk.
State of hydration. Proper hydration is important for general and diving health. Dehydration can increase the risk of DCS, and hyperhydration can promote immersion pulmonary edema. Practically, it is probably fair to say that the diving community has sometimes focused too much on dehydration as a risk factor in decompression stress. This may arise from two realities. First, since fluid shifts and indications of marked dehydration can be a consequence of DCS, there can be some confusion over cause and effect. Second is the human desire to find something simple to blame.
Physical fitness. Divers should be physically fit enough to meet the normal demands of diving with sufficient reserve capacity to handle emergency situations. The higher the level of physical fitness, the lower the relative strain of a dive. Optimal body composition reduces the amount of ballast weight that has to be carried to achieve neutral buoyancy and, in the case of an obligatory postdive climb out, reduces the absolute effort required. Limited data have associated higher levels of physical fitness with reduced postdive bubble formation and lower risk of DCS.
The biggest practical challenge typically arises with efforts to schedule exercise around busy diving schedules. While limited findings suggest that a single bout of high-intensity exercise conducted 24 hours before diving may have a protective effect, the data concerning exercise closer to the start of diving are fairly confusing. Exercise should probably be avoided pre- and postdive where possible.
DCS history. An individual’s history of DCS may indicate a greater predisposition, either physiologically or behaviorally. The importance of history may also extend to a buddy since his or her actions can influence the outcome of a shared activity.
Age. The impact of increasing age is difficult to assess since it may be confounded with reduced levels of physical fitness and changing health and practices. Increasing age is associated with increased bubble formation, and this potentially indicates a reduced tolerance for decompression stress.
Sex. There is no compelling evidence in the diving literature to confirm that sex plays a role in the development of DCS. This runs contrary to a limited amount of data from hypobaric chamber exposures that suggest that the physiological risk may vary somewhat across the menstrual cycle, with a slightly elevated risk during the first half of the cycle. Practically speaking, even if women do have a slightly elevated physiological risk in comparison to males, a tendency toward more conservative practice may reduce the net risk.
Circulation. Compromised circulation resulting from prior injury has been viewed as a possible risk factor, but with little empirical evidence. The presence of a patent foramen ovale (PFO) has the potential to alter circulation by allowing a volume of blood to reach the systemic circulation without undergoing filtration through the lung. PFO has been identified as a risk factor in serious DCS. Perspective is required, though, for while the frequency of PFO is fairly high (about 25 percent of the population), the incidence of serious DCS is low. The degree of patency varies and can be important. PFOs are also not the only way to move bubbles into arterial circulation. Bubbles can cross in the lungs, particularly during exercise (while or after climbing out of the water, for example). Dive profiles that minimize bubble formation provide the greatest protection since there will be no bubbles to cross over.
Biological health. A host of factors falling under the category of biological health may influence decompression stress. Some probably play minor roles, while others may play important roles that have not yet been fully defined. Nutritional status, for example, is important for general health and physical fitness and may influence the biochemical response to decompression stress. Similarly, the potential interaction between drugs and diving is another area with virtually no research data but legitimate concerns. Genetic predisposition and epigenetic expression likely also have importance that is just beginning to receive research attention.
Acclimatization. Acclimatization is defined as adaptive change in response to repeated natural exposure. The effect may be positive or negative. Repetitive diving could influence decompression stress, and not just through the presence of residual inert gas. Positive acclimatization could produce a reduction in the biochemical response — effectively a desensitization that may reduce the magnitude of the insult. Negative acclimatization could produce a heightened response — effectively a sensitization to decompression stress. The published data relevant to diving are conflicting, which may be in part a reflection of how divers dive. The effect of positive acclimatization could easily be masked by patterns of increasing exposure intensity over dives in a series.
Summary
Most personal factors that affect decompression stress can be modified. Maintaining reasonable levels of physical fitness, nutrition, restfulness and hydration all contribute to good health and good diving health. Good health can reduce physical limitations and the need for medication.
When selecting dive buddies, divers should consider compatibility of goals, risk tolerance, skills, knowledge and capabilities. A shared understanding of both risk and best practices can improve operations and readiness.
Thoughtful and well-informed divers know far more than current dive computers about conditions that may affect risk during a dive — and likely they will know far more than dive computers for many years to come. Being conscious in real time of conditions that may alter risk can make it easier to build in appropriate buffers to promote safety. Small changes toward conservatism, when applied across a variety of factors, can enhance safety with little impact on what can be accomplished during a dive.
References
1. Pollock NW. Factors in decompression stress. In: Pollock NW, Sellers SH, Godfrey JM, eds. Rebreathers and Scientific Diving. Proceedings of NPS/NOAA/DAN/AAUS June 16-19, 2015, Workshop. Wrigley Marine Science Center, Catalina Island, CA; 2016; 145-56. Available at: http://www.xray-mag.com/sites/default/files/rebreathers_and_scientific_diving_proceedings_2016.pdf
2. Gerth WA, Ruterbusch VL, Long ET. The influence of thermal exposure on diver susceptibility to decompression sickness. NEDU Technical Report 06-07. November 2007.
© Alert Diver — Q4 Fall 2016